6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa4c32d0000007407000001000500
6go6ckt5b5idvals|999
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Plasma cell leukemia is rare type of multiple myeloma with incidence of less than one case per million of all malignancies and 1-2% of multiple myeloma cases [
1,
2]. It is a type of multiple myeloma in which there is peripheral blood absolute plasma cell count of at least 2×10
9/L and more than 20% plasma cells in the peripheral blood differential white cell count [
3]. In non-secretory myeloma there is no monoclonal protein in either the serum or the urine with immunofixation [
3]. Two-thirds of patients with non-secretory multiple myeloma on immuno-fixation had an elevation of free monoclonal light chains in the serum [
4]. These patients may show a faint band in light chain region without heavy chain band on serum immunofixation electrophoresis. The aim of this case report is to present a challenging case of non-secretory plasma cell leukemia.
Case Report
A 64-year-old male, presented with 2 month history of backache in the mid-dorsal region. He exhibited painful and restricted movements with difficulty in walking. He had past medical history of squamous cell carcinoma of oral cavity seven years back which was treated by hemi-glossectomy, hemi-mandibulectomy and followed by radio and chemotherapy. Patient was recently diagnosed as having hypothyroidism.
The physical examination showed pulse rate: 76/min, respiratory rate: 15/min, blood pressure: 120/70 mm Hg, and mild pallor. Examination of the head, neck, chest, abdomen, upper extremities and skin was unremarkable. Back examination shows local tenderness over D-10, and restricted movements. MRI dorsal spine showed lytic lesions at multiple vertebral levels. PET scan showed hyper-metabolic parenchymal nodule in lower lobe of right lung with multiple lytic lesions involving almost entire axial and appendicular skeleton. Expansile lytic lesions in right 8th, 9th rib with large associated soft tissue component were amenable to sampling. Various tumor markers were reported as PSA: 1.77 ng/mL (normal), CEA: 2.8 ng/mL (normal), CA 19.9: 6 U/mL (normal).
Hematological and biochemical investigations were reported as Hb:11 g/dL, WBC: 88.7×103/µL, neutrophils: 7%, lymphocytes: 9%, eosinophils: 1%, monocytes: 3%, basophils: 0%, platelet: 99×103/µl, RBC: 3.69 million/cumm, Hct: 33.9%, RDW: 19.5%, normal renal function tests, serum protein: 6.8 g/dL, albumin: 4.0 g/dL. Peripheral smear microscopic examination was done which showed hyper-leukocytosis with presence of 87% plasma cells.
Tru-cut biopsy of right chest wall mass lesion showed sheets of small round shaped cells with monomorphic round nucleus, finely granular and scanty eosinophilic cytoplasm, few plasmacytoid cells, and no mitosis. Focus of necrosis was seen. Immunohistochemistry showed CD 138 positive, kappa positive, lambda negative, synaptophysis negative, chromogranin negative, Ki67: 3-4%, and LCA negative.
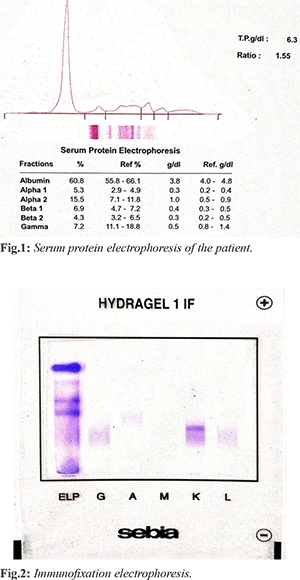
Serum protein electrophoresis [Fig.1] showed hypo-gammaglobunemia and there was no “M” band. Immunofixation electrophoresis [Fig.2] showed a faint band in the kappa region and no corresponding heavy chain was seen. Urine electrophoresis was also normal with no “M” band seen. Serum values were kappa light chain: 25.9 mg/L (raised), lambda light chain: 5.26 mg/L (normal) and K/L ratio: 4.924 (raised).
Bone marrow aspirate showed reduced normal hemopoietic elements and 90% plasma cells. Bone marrow biopsy showed diffuse interstitial increase in plasma cells which present in clusters and sheets. Several mature plasma cells and few immature plasma cells were seen. Normal hemopoietic elements are reduced. On IHC, CD-138 shows clusters and sheets of plasma cells in marrow interstitium, CD-56 was negative. Clinical profile, peripheral smear, bone marrow aspirate and biopsy features were consistent with plasma cell leukemia. FISH myeloma panel was done which showed p53 del negative, del 13q14.3 negative, t(4;14) negative, t(11,14) positive, t(14,16) negative. Treatment of plasma cell leukemia and flow cytometric studies were planned but the patient did not come for follow up.
Discussion
Non-secretory plasma cell leukemia is a rare condition diagnosed on the basis of peripheral smear and bone marrow examination. Serum protein electrophoresis is normal and misguides the physicians. There is absence of monoclonal proteins in the blood as well as in the urine [
1-
5]. Most common cause of absence of monoclonal proteins in serum and urine is rapid intracellular or extracellular destruction [
6].
In our case, the presenting complaint was back pain and initial imaging showed various lytic lesions spine. This was dragging the diagnosis towards secondaries due to some unknown primary tumor present in the body, that could be the recurrence of the squamous cell carcinoma of oral cavity that occurred seven years back or may be due to some other hidden primary carcinoma. Complete blood count and peripheral smear suggested hematological malignancy. Bone marrow aspirate showing 87% plasma cells and normal serum protein electrophoresis pointed to diagnosis of non-secretory plasma cell leukemia. Immunofixation electrophoresis showed a faint band in the kappa region and also in free light chain assay, kappa light chains were slightly raised with raised K/L ratio. These findings were consistent with the literature, in which it is mentioned that two third of patients with plasma cell leukemia show a rise in light chains in serum [
4]. Sureda A et al. also presented a case in which multiple lytic lesions with no “M” band on SPE and it was confused with the secondaries, but the diagnosis was made on peripheral smear and bone marrow aspiration [
7].
Plasma cell leukemia is very aggressive type of multiple myeloma with very poor prognosis with poor response to chemotherapy and median survival of less than one year [
8,
9]. Non-secretory type of plasma cell leukemia is rare condition with only a few cases reported world-wide [
7,
8,
10].
Conclusion
Multiple myeloma cannot be excluded by absence of “M” band in SPE. Though it is not possible to do bone marrow biopsy in all the cases, but when multiple myeloma is suspected, hematologist should always be consulted for the peripheral smear findings to avoid delay in diagnosis.
Contributors: RC wrote the manuscript and was involved in laboratory diagnosis. PJ and AKH critically revised the manuscript for important intellectual contents. RC will act as a study guarantor. All authors have read and approved the final manuscript and are responsible for all aspects of the study.
Funding: None; Competing interests: None stated.
References
- Ramsingh G, Mehan P, Luo J, Vij R, Morgensztern D. Primary plasma cell leukemia. Cancer. 2009;115:5734-5739.
- Prabhat D, Bijur SJ, Pathare AV. Plasma cell leukaemia--a report of two cases. J Postgrad Med. 1998;44-47.
- Kyle RA, Child JA, Anderson K, Barlogie B. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. British J Haematol. 2003;121:749-757.
- Drayson M, Tang LX, Drew R, Mead GP, Carr-Smith H, Bradwell AR. Serum free light-chain measurements for identifying and monitoring patients with non-secretory multiple myeloma. Blood. 2001;97:9.
- Shaw GR. Non-secretory plasma cell myeloma-becoming even more rare with serum free light-chain assay. Arch Pathol Lab Med. 2006;130:1212-1215.
- Decourt C, Galea HR, Sirac C, Cogne M. Immunologic basis for the rare occurrence of true non-secretory plasma cell dyscrasias. J Leukoc Biol. 2004;76:528-536.
- Sureda A, Pais JR, Pascual J, Perez Vaquero MA, Hernando JC. Non-secretory multiple myeloma presenting as primary plasma cell leukaemia. Postgrad Med J. 1992;68:470-472.
- Humeida A, Ihsan M. Osman, Hiba A Awooda, El Tahir MM. Non-secretory primary plasma cell leukemia - A case report. American J Medical Case Reports. 2014;2:266-268.
- Gonsalves WI, Rajkumar SV, Ronald S. Go, Dispenzieri A, Trends in survival of patients with primary plasma cell leukemia: a population-based analysis. Blood. 2014;124:907-912.
- Dadu T, Rangan A, Handoo A, Bhargava M. Primary non-secretory plasma cell leukemia with atypical morphology – a case report. Indian J Hematol Blood Transfus. 2009;25:81-83.