|
|
|
|
|
Giant Acute Extradural Hematoma following Titanium Mesh Cranioplasty
|
|
|
|
Rahul Singh, Ravi Shankar Prasad, Ramit Chandra Singh, Kulwant Singh, Anurag Sahu, Nityanand Pandey Department of Neurosurgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr Ravi Shankar Prasad Email: rsprasadbhuhodneurosurgery@gmail.com |
|
|
|
|
|
|
|
|
Received:
29-JUN-2020 |
Accepted:
13-NOV-2020 |
Published Online:
15-FEB-2021 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: Giant acute extradural hematoma following titanium mesh cranioplasty is very rare. Case Report: We report a giant post-cranioplasty extradural hematoma which required surgical evacuation and removal of titanium implant. The titanium mesh cranioplasty was done for a post-craniectomy defect from right sided decompressive craniectomy for right fronto-temporo-parietal acute subdural hematoma (aSDH) and contusion. On surgical evacuation, patient recovered. Later on repeat titanium mesh cranioplasty was done with no complications. Conclusion: This case report intends to warn against a potential dangerous complication following cranioplasty in the post-operative period that must be kept in mind while doing post-operative care. |
|
|
|
|
|
Keywords :
|
Contusions, Decompressive Craniectomy, Hematoma, Skull, Surgical Mesh, Titanium.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffecca310000006807000001000500 6go6ckt5b5idvals|2050 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Post-operative intracranial hematoma in the form of giant extra-dural hematoma is a rare complication after cranioplasty using titanium mesh in a patient with normal coagulation profile. Only few case reports of such a complication are reported [ 1]. We report a case of giant extra-dural hematoma following titanium mesh cranioplasty that appeared in a patient on second post-operative day due to scalp arterial bleeding.
Case Report
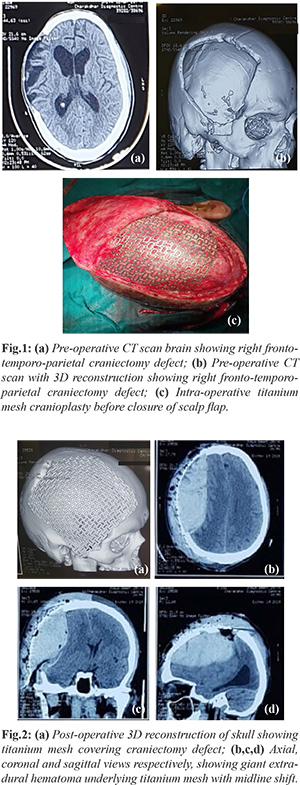
The patient was a 35 year old male who first presented in September 2019 with a Glasgow Coma Scale (GCS) score of 11 following a head injury due to motor vehicle accident. Non-contrast computed tomography (NCCT) scans revealed a right sided fronto-temporo-parietal acute subdural hematoma (aSDH) and right fronto-temporal contusion. After resuscitation, patient was taken to the neurosurgery emergency operation theater and a right sided fronto-temporo-parietal decompressive craniectomy was performed along with a tracheostomy. Bone flap was placed subcutaneously in the abdominal wall. His ICU stay was complicated by ventilator associated pneumonia which resolved on treatment. The patient recovered with the Glasgow outcome score (GOS) of 5 i.e. good recovery with some impairment in cognition. In December 2019, he presented to us with post-craniectomy defect for cranioplasty. His pre-operative coagulation profile was normal with platelet count: 1.5 lakhs/cumm, prothrombin time (PT): 12 seconds, international normalized ration (INR): 1.1, bleeding time: 2.5 minutes and activated partial thromboplastin time (APTT): 36 seconds. No history of any previous bleeding diathesis was present. Pre-operative complete blood count, liver profile, kidney function test were within normal limits. Patient was negative for HIV, HBsAg and HCV viral marker profile. Pre-operative hemoglobin was 13 g/dL. Patient was operated in elective settings and titanium mesh cranioplasty was done for craniectomy defect [Fig.1]. Autologous bone flap placed in abdominal wall was discarded due to its resorption leading to inadequate craniectomy cover. Sub-galeal drain was placed after meticulous hemostasis. Patient was extubated and shifted to post-operative ward. Post-operative CT scan done after 4 hours was satisfactory. Sub-galeal drain was removed on post-operative day (POD) 1. Post-operative blood investigations sent after 12 hours showed normal coagulation profile (hemoglobin 12.2 g/dL, platelet count 1.7 lakhs/cumm, PT 13 sec, INR 1.2, APTT 35 seconds and bleeding time 2.8 minutes). On POD 2, he developed sudden deterioration in Glasgow coma scale (GCS) score from GCS of 15 to GCS of 11. Right pupil was dilated with sluggish pupillary reflexes (both direct and indirect). CT scan showed a huge scalp and extra-dural hematoma and midline shift of 17 mm [Fig.2]. Patient was immediately shifted to emergency OT and surgical evacuation of extra-dural hematoma with removal of titanium mesh was done. Intra-operatively, scalp artery was identified as the bleeding source that through the porous titanium mesh had caused extra-dural hematoma. Subgaleal drain was placed. Post-operatively GCS recovered to 15 and CT scan showed no hematoma. Post-operative period was uneventful. He was discharged on 10th post-operative day. Later in February 2020, a repeat titanium mesh cranioplasty was done with uneventful recovery.
Discussion
Cranioplasty is a procedure performed for reconstruction of craniectomy defects following cranial surgeries or injuries. Cranioplasty is done either in an autologous manner or by using artificial meshes or implants. Accordingly, materials used for cranioplasty can be classified as biological and artificial or synthetic materials [ 2]. In autologous cranioplasty, bones from cranium or from other areas of the body are utilized. Synthetic materials commonly used for cranioplasty are methyl methacrylate (MMA), hydroxyapatite, titanium mesh, alumina ceramics and polyetheretherketone (PEEK) implant [ 3]. At our centre we use titanium mesh for cranioplasty when autologous bone graft is not available or suitable due to resorption or infection. Titanium mesh can either be used alone or it may be combined with MMA or hydroxyapatite for better cosmesis [ 3]. Titanium mesh cranioplasty has better cosmetic results when compared to other synthetic materials as quoted in several studies [ 3, 4]. Moreover, lowest infection rate is seen using titanium implants [ 3, 4]. It is costly and studies have reported it to be heat conductive and it produces imaging artifacts [ 5, 6, 7]. Due to its inert nature, titanium has higher biocompatibility. Hemorrhagic complications following cranioplasty consists of extra-dural hematoma, sub-dural hematoma, intra-cerebral hemorrhage, and extra-axial fluid collections that may require evacuation [8]. Studies have reported the hemorrhagic complications range from 2.5-7.5% [ 9, 10]. However, giant extradural hematoma following cranioplasty is only reported in few case reports [ 1]. In our case, source of bleeding was scalp artery. Due to permeable nature of mesh, the blood percolated through it and caused the extra-dural collection. Due to slow development of extra-dural hematoma (EDH), neurological deterioration was delayed. Titanium mesh cannot be attributed as the cause of EDH in our case and we do not discourage the use of titanium mesh for cranioplasty. This case report intends to warn against a potential dangerous complication following cranioplasty in the post-operative period that must be kept in mind while doing post-operative care. Moreover, coagulation profile of the patients planned for cranioplasty must be evaluated both pre-operatively and post-operatively to rule out any bleeding diathesis which may theoretically result in such complication.
Conclusion
Hemorrhagic complications following titanium mesh cranioplasty are rare if proper hemostasis is achieved intra-operatively. Scalp hemostasis should be typically cared of as it may result in gradual development of giant EDH leading to rapid deterioration of neurological status. Post-operative neurological monitoring and care is essential for early detection and management of such complication.
Contributors: RS, RSP: Manuscript writing, literature review and patient management; RCS, KS: reviewing the literature and manuscript editing; AS, NP: critical inputs into the manuscript. RSP will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of the study. Funding: None; Competing interests: None stated.
References - Martin MP, Olson S. Post-operative complications with titanium mesh. J Clin Neurosci. 2009;16(8):1080-1081.
- Alkhaibary A, Alharbi A, Alnefaie N, Aloraidi A, Khairy S. Cranioplasty: A comprehensive review of the history, materials, surgical aspects and complications, World Neurosurgery. 2020;139:445-452.
- Shah AM, Jung H, Skirboll S. Materials used in cranioplasty: a history and analysis. Neurosurg Focus. 2014;36(4):E19.
- Matsuno A, Tanaka H, Iwamuro H, Takanashi S, Miyawaki S, Nakashima M, et al. Analyses of the factors influencing bone graft infection after delayed cranioplasty. Acta Neurochir (Wien). 2006;148(5):535-540.
- Cabraja M, Klein M, Lehmann TN. Long-term results following titanium cranioplasty of large skull defects. Neurosurg Focus. 2009;26(6):E10.
- Wiggins A, Austerberry R, Morrison D, Ho KM, Honeybul S. Cranioplasty with custom-made titanium plates 14 years experience. Neurosurgery. 2012;72(2):248-256.
- Wind JJ, Ohaegbulam C, Iwamoto FM, Black PM, Park JK. Immediate titanium mesh cranioplasty for treatment of post-craniotomy infections. World Neurosurg. 2013; 79(1):207.e11-3.
- Hng D, Bhaskar MI, Khan FM, Budgeon C, Damodaran O, Knuckey N, et al. Delayed cranioplasty: outcomes using frozen autologous bone flaps. Craniomaxillofac Trauma Reconstr. 2015;1:190-197.
- Bender A, Heulin S, Röhrer S, Mehrkens JH, Heidecke V, Straube A, et al. Early cranioplasty may improve outcome inneurological patients with decompressive craniectomy. Brain Inj. 2013;27:1073-1079.
- Piedra M, Nemecek A, Ragel B. Timing of cranioplasty after decompressive craniectomy for trauma. Surg Neurol Int. 2014;5:25.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Singh R, Prasad RS, Singh RC, Singh K, Sahu A, Pandey NGiant Acute Extradural Hematoma following Titanium Mesh Cranioplasty.JCR 2021;11:32-34 |
|
Singh R, Prasad RS, Singh RC, Singh K, Sahu A, Pandey NGiant Acute Extradural Hematoma following Titanium Mesh Cranioplasty.JCR [serial online] 2021[cited 2026 May 21];11:32-34. Available from: http://www.casereports.in/articles/11/1/Giant-Acute-Extradural-Hematoma-following-Titanium-Mesh-Cranioplasty.html |

|
|
|
|
|