6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff6c03330000008706000001000b00
6go6ckt5b5idvals|3064
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Calcium absorption and regulation involve a complex interplay between multiple organ systems and regulatory hormones. The three predominant sources of calcium and targets for regulation are the bones, renal filtration and reabsorption, and intestinal absorption. The major regulators of calcium levels are parathyroid hormone (PTH) and vitamin D, which target the bones, intestine, and kidney to increase serum calcium [
1]. Infants and children are in a state of high bone turnover. Therefore, they are prone to the imbalance of osteoblastic and osteoclastic activity that occurs with prolonged immobilization, leading to hypercalcemia [
2]. Immobilization hypercalcemia diagnosis requires an evaluation to rule out hypercalcemia causes. Cancer associated hypercalcemia should be excluded, if guided by clinical suspicion [
3].
Albright et al. presented a 14-year-old boy who developed hypercalcemia and hypercalciuria after being immobilized secondary to a femoral neck fracture. The mechanism underlying immobility-induced hypercalcemia relates to the loss of balance between osteoblastic bone formation and osteoclastic bone resorption [
4]. Several characteristic predisposing factors emerge from a study of later reports. The affected patients have all been boys between the ages of nine and fifteen years. Most patients have sustained fractures, often multiple, of their long bones requiring prolonged periods of immobilization [
5].
Case Report
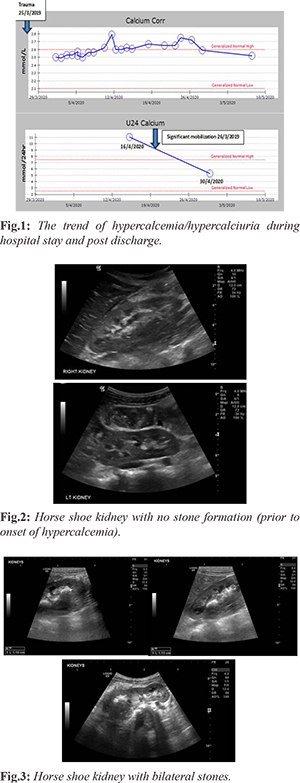
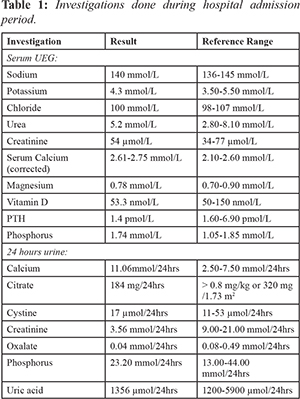
A previously healthy 10 years old male was admitted with blunt abdominal trauma after motor vehicle collision. Imaging revealed hollow viscous perforation, pancreatic body and tail contusion with surrounding hematoma, left kidney contusion, and grade I hepatic injury. He underwent exploratory laparotomy on day 1 with gastrorrhaphy repair of gastric perforation and extensive washout. The child remained in intensive care for 16 days, and suffered major complication including pancreatitis secondary to the abdominal trauma for which he received octreotide infusion and total parental nutrition. His calcium levels started to increase on day 15 post-operatively [Fig.1]; pancreatitis improved initially then deteriorated secondary to the development of the new onset mild hypercalcemia. He also developed macroscopic hematuria with hypercalciuria, imaging revealed 4×4 mm left vesicoureteral renal stone [Fig.2,3]. Stone studies showed calcium oxalate stone. He continued to have hypercalcemia despite being on hyperhydration, he was only kept on urinary alkalization treatment; hydrochlorothiazide was deferred until correction of hypercalcemia. His serum calcium level remained high for 17 days. He also needed another course of octreotide infusion to decrease his pancreatic enzymes.
Hematuria recurred few times during this period and repeated imaging after 12 days revealed new right renal stone 1.3 cm. The etiology of hypercalcemia was investigated; he had unremarkable past medical history, strong family history of renal stones, PTH and vitamin D levels were measured, which showed a normally-suppressed PTH and normal vitamin D levels. After exclusion of other differential diagnosis, the cause of his hypercalcemia was limited to prolonged immobilization. Management mainly included proper hydration, low calcium diet, in addition to encouraging early mobilization. His calcium level gradually corrected especially after being discharged home, and he was followed up in outpatient setting until calcium level normalized. Repeated KUB ultrasound was unremarkable for renal stones.
Discussion
Immobilization hypercalcemia is an uncommon diagnosis predominately present in children or young adults with limited mobility during the first four to six weeks after the precipitating injury/immobilization; nevertheless, it can present even months after [
6]. The diagnosis of immobility induced hypercalcemia in our patient was made after the exclusion of the other common causes of hypercalcemia. As he had prolonged hospital stay with limited mobility secondary the motor vehicle accident and operative intervention, his immobilization reached up to four weeks, therefore the entity of immobilization induced hypercalcemia was considered. Hypercalcemia may occur during prolonged immobilization in any condition associated with increased bone turnover.
In the healthy individual there is a balance between the resorption and the formation of bone which is influenced by age, nutritional and hormonal factors as well as the degree of physical activity. Osteoblastic activity is thought to be stimulated by mechanical stress. If such stress is removed by immobilization, then bone formation is reduced, leaving a relative excess of bone destruction causing the release of calcium into the extracellular fluid. Under normal circumstances, this increase in extracellular calcium concentration is compensated by increased urinary calcium excretion maintaining normal serum calcium concentrations [
5].
Hypercalcemia related to immobilization was first described by Albright et al. [
4], in 1941. Another case reported described two boys (11 and 14 years old), who were immobilized with peripheral neuropathy developed hypercalcemia which was attributed to immobility [
5]. Most of the cases were described in adult patients, however it was noted that this condition is more common in children and adolescents in whom bone turnover is high. One literature described a rare case of immobility-induced hypercalcemia in a 2-month-old female infant [
2]. The management of hypercalcemia depends on the level of severity. Our patient had mild hypercalcemia
[Table 1]. The management was mainly hydration with intravenous normal saline and mobilization. Fluids expand the extracellular fluid volume, which increases the glomerular filtration rate, and increases the excretion of calcium in the urine.
In our patient, pancreatitis was worsening. This was evident by an increase in pancreatic enzymes less than 24 hours after hematuria onset. We think that the hypercalcemia played a role into this, although other causes like a small pseudocyst and the pancreatic injury were also present. Pancreatic enzymes improved further after controlling the serum calcium despite the presence of the pseudocyst. Nephrolithiasis was investigated and stone studies were done on 2 occasions, no reason was found apart from hypercalciuria. After the mobilization and the subsequent resolve of hypercalcemia, a 24 hrs urine collection showed normalization of the previous hypercalciuria [Table 2].
Conclusion
Prolonged immobilization has been associated with hypercalcemia and hypercalciuria in adolescents and younger adults. Its prevalence in pediatric population has not been commonly reported. It usually occurs as a result of imbalance in bone remodeling leading to excessive mobilization of calcium to the blood. Complications like kidney stones formation and pancreatitis may happen as well especially if we didn’t pay an attention and this may lead to morbidities and may extend the hospital stay.
Contributors: AMA: manuscript writing, patient management; TA: manuscript editing, patient management; AAS: critical inputs into the manuscript. AMA will act as guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study.
Funding: None; Competing interests: None stated.
References
- Pitukcheewanont P, Nakamoto J. Pediatric Hypercalcemia. Emedicine.medscape.com. Available from: https://emedicine.medscape.com/article/920955-Overview. Accessed on October 28, 2020.
- Vyas, N, Kaminski, B, MacLeish S. A rare case report of immobility-induced hypercalcemia in an infant. Pediatrics. 2016;137: e20150879.
- Cano-Torres E, González-Cantú A, Gabriela Hinojosa-Garza G, Castilleja-Leal F. Immobilization induced hypercalcemia. Clin Cases Miner Bone Metab. 2016;13(1):46-47.
- Albright F, Burnett CH, Cope Q, Parson W. Acute atrophy of bone (Osteoporosis) simulating hyperparathyroidism. J Clin Endocrinol. 1941;1:711-716.
- Walls TJ, Ashworth B, Saunders M. Immobilisation hypercalcaemia complicating polyneuropathy in adolescent boys. Journal of Neurology, Neurosurgery & Psychiatry. 1984;47:1232-1235.
- Reynaga BM, Zeni SN. Marcadores bioquímicos del remodelamiento óseo. Utilidad clínica. Acta Bioquim Clin Latinoam. 2009;43(2):177-193.