|
|
|
|
|
Solitary Colon Metastasis from Renal Cell Carcinoma
|
|
|
|
Arjav H Nanavati, Jenny Thomas, Priya Barbaniya, Rajeshkumar C Mahey, Sudatta B Waghmare Department of General Surgery, TNMC & BYL Nair Ch. Hospital, Mumba, Maharashtra, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr Sudatta Waghmare Email: sudattaw@gmail.com |
|
|
|
|
|
|
|
|
Received:
26-OCT-2020 |
Accepted:
08-OCT-2021 |
Published Online:
15-NOV-2021 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: The most common renal malignancy in adults is renal cell carcinoma (RCC). Metastatic disease is relatively common and at the time of diagnosis may be present in upto 25% of patients. Frequent sites of metastasis are lung, bone, brain, liver and adrenal glands. The risk of recurrence even after curative resection is a 30-40%. The gastrointestinal tract, particularly the colon, represents a very uncommon site of late metastatic disease. Case Report: We present a case of a 40-year-old-male with solitary colonic renal cell carcinoma metastasis. Patient underwent laparoscopic nephrectomy in 2016 in view of renal mass and was followed by chemotherapy for clear cell carcinoma. He had history of water diarrhoea, abdominal pain, tenesmus and haematochezia. Investigation revealed circumferential thickening involving the proximal and mid segment of sigmoid colon, stricture around 30 cm from the anal verge and histopathology suggestive of deposits of renal cell carcinoma. FDG PET scan was suggestive of enhancing necrotic lesion in the wall of sigmoid colon with multiple deposits noted in adjacent mesentery. On diagnostic laparoscopy focal lesion was noted in the sigmoid colon with no evidence of omental, peritoneal and any other metastasis. Resection and anastomosis of lesion was done. Histopathology was clear cell carcinoma with clear margins. Conclusion: The colon is a potential, though uncommon, site for solitary metastasis from RCC. Oncologic resection with negative margins may result in long-term survival in patients with isolated metastatic disease. |
|
|
|
|
|
Keywords :
|
Colonic Diseases, Metastasis, Renal Cell Carcinoma, Sigmoid Colon, Solitary Kidney.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa810360000008f06000001000f00 6go6ckt5b5idvals|3100 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Renal cell carcinoma (RCC) is the most common renal malignancy and represents approximately 3% of malignant tumors in adults. The most frequent histological type is clear cell carcinoma. In patients with localized disease surgical resection remains the primary curative treatment. Nearly 40% of patients will develop metastasis even after nephrectomy. The most common sites of metastasis are the lung, liver, bone, and brain [ 1], whereas metastasis to the gastrointestinal tract, specifically the colon, is extremely rare. We report a case of a patient who presented with a late recurrence of RCC in the sigmoid colon and was treated successfully with colonic resection.
Case Report
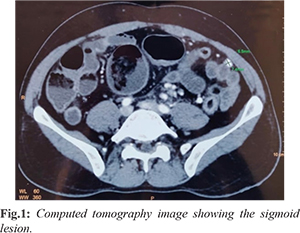
The patient is a 40-year-old male who underwent laparoscopic nephrectomy for left renal mass in 2016. The histopathology was suggestive of clear cell carcinoma of the left kidney grade T2a. Patient was started on tab sunitinib 50 mg for 1 year. He subsequently presented in out-patient department with complaints of watery diarrhoea, abdominal pain, tenesmus, haematochezia. Patient was vitally stable maintaining normal pulse, blood pressure, temperature and oxygen saturation. Per abdomen was soft, non-tender, but distended and per rectum, anal tone was normal. X-ray and ultrasound didn’t show any significant findings. Computed tomography scan showed circumferential thickening involving proximal and mid segment of sigmoid colon [Fig.1]. The patient underwent colonoscopy, which revealed a tight stricture with surrounding edema at 30 cms from anal verge. Scope could not be negotiated beyond the stricture. Multiple biopsies were taken. Histopathology report of which was suggestive of deposits of clear cell renal cell carcinoma. FDG PET scan was suggestive of FDG avid heterogeneously enhancing necrotic lesion in the wall of sigmoid colon measuring 2.7×3.3 cm with multiple deposits noted in adjacent mesentery.
Patient was posted for elective diagnostic laparoscopy. There was focal lesion at sigmoid colon without any liver, omental and peritoneal deposits. Hence decision was taken to go ahead with sigmoid resection and anastomosis [Fig.2]. Post-operative recovery was uneventful. Histopathology showed deposit from RCC with margins free from tumor [Fig.3].
Discussion
We reported a case of metastatic RCC to sigmoid colon. The patient had symptoms associated with colonic lesions, like watery diarrhoea, tenesmus, haematochezia. On colonoscopy and FDG PET/CT images, hyper-metabolic activity in sigmoid colon was noted. Histopathology confirmed metastasis from RCC. Few cases of metastatic RCC to rectum or colon have been reported. One of them, presented with haematochezia after receiving a left nephrectomy for RCC and was found to have a sub-mucosal mass with ulcerated area in rectum by colonoscopy and ultrasound [ 1]. The other patient with metastatic RCC to rectum directly received surgery, without any endoscopy or imaging [ 2]. The mechanism of metastasis of RCC is still unclear, but the blood supply and thin tissue of rectum may be not appropriate for the development of RCC, compared with common metastatic sites such as lungs. The high malignancy and strong invasive ability of tumor may have led to rectal metastasis, as the presence of such a rare metastatic site of RCC usually indicates relatively poor prognosis. Other unusual metastatic sites of RCC include colon, intestine, stomach, pancreas, gallbladder, prostate, thyroid gland, and skeletal muscle [ 3- 7]. These rare metastatic sites were usually accompanied by multiple metastasis in the whole body, over the period from the initial diagnosis of RCC to metastasis from several years to more than 10 years. In this report, FDG-PET/CT images of metastatic RCC in rectum showed hyper-metabolic activity in sigmoid colon. Higher SUV usually indicates higher malignancy of tumors, invasiveness nature of tumor cells, and worse prognosis of patients. The metastasis of other sites such as bilateral lungs and right ilium can be evaluated predicting the patient condition and its prognosis. hence important for surveillance. Therefore, FDG-PET/CT is a valuable examination for appropriate case in order to increase the concern about metastatic disease and to influence further evaluation and management [ 8] because it could efficiently detect small lesions and identify malignant cases.
Conclusion
Regular examinations and strict follow-up after nephrectomy are necessary for patients with diagnosis of RCC. Rectum and other unusual metastatic sites of RCC should not be ignored in surveillance on RCC.
Contributors: AHN, JT: manuscript writing and patient management; PB, RCM: manuscript editing and patient management; SBW was involved in providing critical inputs, patient management and will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study. Funding: None; Competing interests: None stated.
References - Dellon ES, Gangarosa LM. Haematochezia due to a renal cell carcinoma metastasis to the rectum: a case report and review of the literature. Rev Gastroenterol Mex. 2006;71:316-318.
- Rosito MA, Damin DC, Lazzaron AR, André C, Schwartsmann G. Metastatic renal cell carcinoma involving the rectum. Int J Colorectal Dis. 2002;17:359-361.
- Chetty R, Syed A, van der Kwast T. Metastatic clear cell renal cell carcinoma presenting as multiple colonic polyps. Int J Surg Pathol. 2011;19:791-794.
- Brener ZZ, Zhuravenko I, Jacob CE, Bergman M. An unusual presentation of renal cell carcinoma with late metastases to the small intestine, thyroid gland, nose and skull base. Nephrol Dial Transplant. 2007;22:930-932.
- Riviello C, Tanini I, Cipriani G, Pantaleo P, Nozzoli C, Poma A, et al. Unusual gastric and pancreatic metastatic renal cell carcinoma presentation 10 years after surgery and immunotherapy: a case report and a review of literature. World J Gastroenterol. 2006;12:5234-5236.
- King DH, Centeno AS, Saldivar VA, Sarosdy MF. Renal cell carcinoma metastatic to the gallbladder or prostate: two case reports. Urology. 1995;46:722-725.
- Lohiya V, Lohiya S, Windsor K. A large thigh mass: a blood clot or a rare skeletal muscle metastasis from renal cell carcinoma. Springerplus. 2013;2:399.
- Bouchelouche K, Oehr P. Positron emission tomography and positron emission tomography/computerized tomography of urological malignancies: an update review. J Urol. 2008;179:34-45.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Nanavati AH, Thomas J, Barbaniya P, Mahey RC, Waghmare SBSolitary Colon Metastasis from Renal Cell Carcinoma.JCR 2021;11:225-227 |
|
Nanavati AH, Thomas J, Barbaniya P, Mahey RC, Waghmare SBSolitary Colon Metastasis from Renal Cell Carcinoma.JCR [serial online] 2021[cited 2026 Mar 31];11:225-227. Available from: http://www.casereports.in/articles/11/4/Solitary-Colon-Metastasis-from-Renal-Cell-Carcinoma.html |

|
|
|
|
|