6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa481380000006807000001000700
6go6ckt5b5idvals|3128
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
A silent aortic thrombus presenting as hoarseness is a rare clinical condition. Tumors of the lung, oesophagus and thyroid are the most common causes of vocal cord paralysis. Vocal cord paralysis may result from the complications of cardiovascular diseases like mitral stenosis, pulmonary artery hypertension, patent ductus arteriosus and atrial septal defect. Impaired function of the nerve could be due to stretching or compression of the nerve due to the enlargement of the aortic vessel at the site where the nerve passes.
Case Report
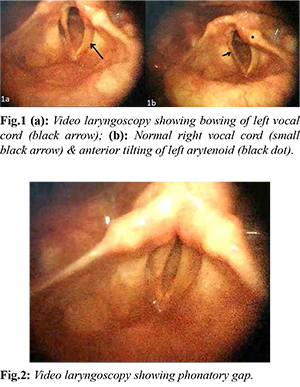
A 70-year-old male patient presented to our outpatient department with complaints of hoarseness of voice for the last three months. It was insidious in onset and progressively worsened with time. There was no history of dyspnoea, dysphagia, odynophagia, symptoms of aspiration or any neck swelling. There was no history of any known co-morbidities. On indirect laryngoscopy, the patient had left vocal cord palsy with the cord in the intermediate position. There was bowing of left vocal cord [Fig.1a] and which was at a higher level than the right vocal cord. The left arytenoid cartilage was tilted anteriorly [Fig.1b] with a persistent phonatory gap [Fig.2]. There were no signs of aspiration and no evidence of any local cause of vocal cord palsy. Rigid laryngoscopy revealed left vocal cord palsy. The right cord was mobile. Swallowing evaluation showed only minimal aspiration with a PAS score of 2. The radiological examination was done to rule out the causes of unilateral left vocal cord palsy including ultrasonography of the neck which showed no thyroid gland pathology or neck nodes. Computed tomography (CT) of the neck showed features of left vocal cord paralysis without any other regional abnormality.
Contrast enhanced CT of the thorax revealed revealed a 5.4×5×7 cm silent thrombus in the arch of aorta extending into ascending aorta [Fig.3b; red dot] The patient did not have any cardiac symptoms or symptoms of vascular compromise. The results of cardiac auscultation and electrocardiography were normal. Then the patient was referred to a cardiothoracic surgeon for further evaluation. Patient underwent a stenting of the aortic arch with left subclavian artery bypass.
Discussion
Hoarseness is a common symptom seen by the otolaryngologist. Causes for vocal cord paralysis are divided into supranuclear (lesions involving nucleus ambiguous and supra-nuclear tracts) and infra-nuclear (main trunk of vagus or recurrent laryngeal nerve) [
1]. Of all the causes, peripheral neuropathy is the most common cause for unilateral cord palsy. Unilateral vocal cord palsy causes approximately 48% of all vocal cord paralysis [
2]. It presents with a breathy voice with aspiration, dysphonia and sometimes dyspnoea. Left recurrent laryngeal nerve is more vulnerable to palsy due to its course into the mediastinum and incudes cardiovascular causes, mediastinal masses, or intrathoracic surgery.
On the right side, the vagus nerve crosses the first part of the subclavian artery to enter the thorax. Right recurrent laryngeal nerve arises from the vagus nerve in front of the first part of the subclavian artery where it winds behind the common carotid artery and ascends into the neck. The left vagus nerve enters the thorax between the left common carotid artery and the left subclavian artery. Left recurrent laryngeal nerve arises from the main trunk of the vagus in the mediastinum anterior to the aortic arch, loops around arch lateral to ligamentum arteriosum and courses cranially and medially towards the larynx in the tracheoesophageal groove where it is intimately related to the medial surface of the thyroid gland before it passes under the lower border of inferior constrictor muscle. It enters the larynx behind the articulation of inferior cornu of thyroid cartilage and cricoid cartilage. Around 11% of patients present with hoarseness due to idiopathic causes, including cardio vocal syndrome [
3].This term describes recurrent laryngeal nerve palsy due to any cardiovascular disease [
4]. It was initially described by Ortner in 1897 as nerve palsy due to left atrial enlargement secondary to mitral stenosis. Many case reports have been published highlighting this cardiac cause. To the best of our belief, this picture of aortic thrombus causing vocal palsy has not been reported.
Aortic arch thrombus can occur in a normal or minimally atherosclerotic vessel [
5]. This is a rare disease that usually presents with symptoms of distal embolism to the axillary artery or iliac vessels. It usually presents with life-threatening cardiovascular events with distal embolization into cerebral, visceral, or peripheral areas with significant morbidity and mortality. Hoarseness is an exceedingly rare presenting complaint given the fact that many times the diagnosis would be made serendipitously.
Aortic thrombus is commonly seen in aortic aneurysm and aortic dissection [
6]. However, thrombosis in a healthy aorta is very rare because the high velocity of blood flow that prevents clotting from happening [
7]. Thrombus formation in a healthy aorta may follow atrial fibrillation and other arrhythmias. Our patient's ECG and echocardiography did not reveal any such pathology. Hyper-coagulable states like essential thrombocytosis and protein C deficiency can also result in a similar presentation. In our patient, there was no family history of vascular disorders or significant history suggestive of vascular disorders. The investigation also did not reveal any such presentation.
Vocal cord palsy resulting from an aortic arch thrombus is a rare phenomenon. It occurs due to the compression of the recurrent laryngeal nerve in the aortopulmonary window which is the space between the pulmonary artery and ligamentum arteriosum. Previous autopsy studies have shown the distance between the aorta and pulmonary artery within the aortic window is only 4 mm and is a potential space of nerve compression [
8,
9].
CT angiography followed by trans-oesophageal echocardiography is mandatory for diagnosis of aortic arch thrombosis. Various treatment modalities like anti-thrombolysis and surgery exist for the management of aortic thrombus. Conservative management should be considered in high risk and surgically unfit patients. Few cases have been reported of the recovery of vocal cord palsy in cardio-vocal syndrome after treating underlying cardiovascular disease but it usually depends on the degree and duration of nerve injury [
9].
Conclusion
Aortic arch thrombus should be ruled out and considered as one of the causes of isolated left recurrent laryngeal nerve palsy. Hoarseness may recover once the underlying pathology has been treated provided no further damage to the nerve occurs. Early diagnosis and intervention help in the reversal of hoarseness and preventing serious life-threatening thromboembolic events.
We highlight this rare cause of unilateral left vocal cord palsy which has to be kept in mind when all common causes have been ruled out. The patient presented to us with only hoarseness as the primary complaint but was finally diagnosed to have a slow-growing asymptomatic thrombus that is potentially life-threatening.
Contributors: ST: manuscript writing, literature review; AA: manuscript editing and review; SKS: critical inputs into the manuscript and critical review. AA will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study.
Funding: None; Competing interests: None stated.
References
- Chen RF, Lin CT, Lu CH. Ortner's syndrome a rare cause of unilateral vocal cord paralysis: a case report. Kaohsiung J Med Sci. 2009;25:203-206.
- Blackmore K. Vocal cord paralysis. In: Monnier P, editor. Pediatric Airway Surgery: management of laryngotracheal stenosis in infants and children. Berlin, Heidelberg: Springer Science & Business Media: 2010;pp.107-118.
- Loughran S, Alves C, MacGregor FB. Current aetiology of unilateral vocal fold paralysis in a teaching hospital in the West of Scotland. J Laryngol Otol. 2002;116:907-910.
- Annema JT, Brahim JJ, Rabe KF. A rare cause of Ortner’s syndrome (cardiovocal hoarseness). Thorax. 2004;59:636.
- Okoronkwo NO, Wang F, Di Luozzo G. Ascending and aortic arch thrombus: Cause of myocardial infarction and lower extremity ischemia. J Med Cases. 2015;6:156-158.
- Sohn V, Arthurs Z, Andersen C, Starnes B. Aortic thrombus due to essential thrombocytosis: strategies for medical and surgical management. Ann Vasc Surg. 2008;22:676-680.
- Fayad ZY, Semaan E, Fahoum B, Briggs M, Tortolani A, D’Ayala M. Aortic mural thrombus in the normal or minimally atherosclerotic aorta. Ann Vasc Surg. 2013;27:282-290.
- Chan P, Lee CP, Ko JT, Hung JS. Cardiovocal (Ortner’s) syndrome left recurrent laryngeal nerve palsy associated with cardiovascular disease. Eur J Med. 1992;1:492-495.
- Mulpuru SK, Vasavada BC, Punukollu GK, Patel AG. Cardiovocal syndrome: a systematic review. Heart, Lung and Circ. 2008;17:1-4.