6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff645c390000005707000001000300
Introduction
Tumor lysis syndrome (TLS) is an oncological emergency characterized by metabolic and electrolyte imbalances occurring due to lysis of tumor which is usually seen after cytotoxic treatment. Tumor lysis leads to immediate release of large amounts of various intracellular components. It is associated with hyperuricemia, hyperkalemia, hyperphosphatemia and hypocalcemia. These electrolyte imbalances causes organ dysfunction which are life threatening with acute renal failure and even fatal cardiac arrhythmia and death [
1]. Tumor lysis syndrome develops usually after initiation of chemotherapy but rarely may arise spontaneously before antitumor therapy. TLS is common in patients with hematologic malignancies with high tumor burden but rarely seen in patients with solid tumors [
2]. Here we present a case of spontaneous tumor lysis syndrome in a localized solid tumor associated with hypercalcemia and hyperleukocytosis.
Case Report
A 73 years old lady with a history of type 2 diabetes mellitus and hypertension was diagnosed with carcinoma right breast and underwent right modified radical mastectomy 22 years back. She presented with history of lump in the left breast and left infraclavicular region for 20 days. Physical examination revealed an ill-defined thickening measuring 2×2 cm in the retro-areolar region of left breast with nipple retraction and another tender, hard mass measuring 10×10 cm in the left infraclavicular region.
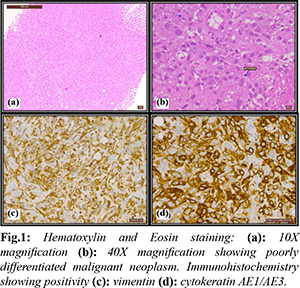
Mammogram and ultrasound of breasts revealed a 13 mm breast imaging-reporting and data system (BI-RADS) IV lesion in the left breast and a large hypoechoic lesion of size 95×73 mm in the left infraclavicular region and axilla. An ultrasound guided core needle biopsy was performed from the left breast lesion and the infraclavicular swelling. Left breast lesion showed proliferative breast disease with intraductal papillomatosis, infraclavicular mass revealed poorly differentiated malignant neoplasm suggestive of carcinosarcoma. Immunohistochemistry (IHC) showed c-expression of pancytokeratin (CK-AE1/AE3) and vimentin in favour of sarcomatoid carcinoma [Fig.1].
18-fluoro deoxy glucose positron emission tomography-computed tomography (PET-CT) showed intense uptake (Standardized Uptake Value max-10.2) with central necrosis in left infraclavicular region and axilla of size 113×105 mm. No infiltration into surrounding muscles and elsewhere in the body was noticed [Fig.2]. Two weeks from biopsy, she presented to emergency department with history of decreased food intake and altered sensorium. She was drowsy, not obeying commands. There was no history of fever or history suggestive of any other focus of infection. There was no history of tumor directed treatment. Her initial investigation revealed elevated blood glucose, creatinine, ketones, uric acid, phosphate, calcium, total leukocyte count, C reactive protein, procalcitonin and lactate dehydrogenase with low bicarbonate. A provisional diagnosis of diabetic ketoacidosis, tumor lysis syndrome and sepsis was made.

She was admitted and managed for tumor lysis syndrome and probable sepsis with intravenous antibiotics cefaperazone and sulbactam, fluids and rasburicase. Her blood and urine culture did not show any growth. She did not have any episodes of fever. Gradually her electrolytes normalised. Inspite of biochemical improvement, she deteriorated clinically. Bone marrow aspiration and biopsy revealed moderately hypercellular marrow with myeloid hyperplasia and shift to left in maturation [Fig.3]. She was started on steroids and hydroxyurea but leukocytosis persisted. Clinically infraclavicular mass became ill defined and softer. Her general condition continued to deteriorate and the patient succumbed 7 days after admission before any tumor directed treatment could be started.
Discussion
This case report describes a 73-year-old woman with a history of type 2 diabetes mellitus and hypertension who presented with a lump in her left breast and left infraclavicular region. Physical examination revealed an ill-defined thickening in the retro-areolar region of the left breast with nipple retraction and a tender, hard mass in the left infraclavicular region. She developed spontaneous lysis syndrome with hypercalcemia and hyperleukocytosis. Biopsy revealed proliferative breast disease with intraductal papillomatosis and poorly differentiated malignant neoplasm suggestive of carcinosarcoma, with immunohistochemistry showing co-expression of pan-cytokeratin and vimentin in favour of sarcomatoid carcinoma. PET-CT showed intense uptake with central necrosis in the left infraclavicular region and axilla. To our knowledge there is no report of a TLS due to localised sarcomatoid carcinoma. According to Cairo Bishop definition, our case meets the criteria for laboratory TLS as well as clinical TLS grade III [
3]. TLS is usually seen in tumors with a high proliferation rate, high tumor burden and pronounced sensitivity to chemotherapy. It is rare to occur in a solid tumor spontaneously. However, there are few case reports of spontaneous TLS in lung, seminoma, gastrointestinal and uterine cancers with high volume disease [
4].
This case highlights the challenges in managing a patient with multiple co-morbidities and advanced-stage cancer. The presence of diabetes mellitus and hypertension can complicate the management of cancer and increase the risk of complications such as diabetic ketoacidosis. Additionally, the development of tumor lysis syndrome, a potentially life-threatening complication of cancer treatment, underscores the need for close monitoring and timely intervention. The diagnosis of carcinosarcoma is also significant as this rare malignancy has a poor prognosis and can be difficult to treat. The co-expression of pancytokeratin and vimentin, as shown by immunohistochemistry, is suggestive of sarcomatoid carcinoma, which is known to be particularly aggressive and resistant to chemotherapy. The patient's rapid clinical deterioration and lack of response to steroid and hydroxyurea therapy highlight the need for more effective treatment options for this rare and aggressive malignancy.
Conclusion
This case report describes a rare occurrence of spontaneous tumor lysis syndrome, accompanied by hypercalcemia and reactive hyperleukocytosis, ultimately resulting in a fatal outcome, in a patient with localized sarcomatoid carcinoma.
Contributors: AE, ANC: Patient care, data acquisition and drafting of the manuscript. RGVR: histopathology and critical inputs into the manuscript. AE will act as a study guarantor. All authors approved the final version of this study and are responsible for all aspects of the study.
Funding: None; Competing interests: None stated.
References
- Mughal TI, Ejaz AA, Foringer JR, Coiffier B. An integrated clinical approach for the identification, prevention, and treatment of tumor lysis syndrome. Cancer Treat Rev. 2010;36(2):164-176.
- Baeksgaard L, Sørensen JB. Acute tumor lysis syndrome in solid tumors-a case report and review of the literature. Cancer Chemother Pharmacol. 2003;51(3):187-192.
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004;127(1):3-11.
- Mirrakhimov AE, Ali AM, Khan M, Barbaryan A. Tumor lysis syndrome in solid tumors: an up-to-date review of the literature. Rare Tumors. 2014;6(2):68-76.