Introduction
Intestinal obstruction constitutes a significant clinical challenge, representing 20% of emergency hospital admissions attributed to acute abdominal pain [1]. Predominantly, adhesional small bowel obstruction takes precedence in these cases. However, a subset of cases involves internal hernias, characterized by the protrusion of abdominal viscera into the abdominal or pelvic cavity through peritoneal or mesenteric defects. Notable variants include para-duodenal, peri-caecal, trans-mesenteric, supra-vesical, peri-vesical, inter-sigmoidal, through the foramen of Wilmslow, trans-omental, and pelvic hernias, each associated with elevated mortality rates [2]. Historically, broad ligament hernias were initially documented in cadaveric specimens in 1861 [3-5], emerging as the most prevalent type of pelvic internal hernias, accounting for 4-7% of all internal hernias [6]. This specific herniation occurs as small intestinal loops become incarcerated within the broad ligament, protruding through defects that may be congenital or secondary in nature (e.g., acquired conditions such as surgery, pelvic inflammatory disease, or obstetric trauma) [2,7].
This study seeks to clarify the management strategies employed in two cases of small bowel obstruction attributed to broad ligament hernias and enhance our understanding of effective management approaches.
Case Report
Case 1
A 42-year-old woman sought emergency care with a 5-day history of abdominal pain, accompanied by vomiting and constipation. Despite a past medical history of depression, she was otherwise in good health, presenting with a mildly distended, soft, and non-tender abdomen. Clinical observations, including the Early Warning Score (EWS), and blood tests were within normal ranges. An empty rectum was noted on examination. Plain abdominal X-ray revealed features indicative of small bowel obstruction, prompting a subsequent abdominal and pelvic CT scan. The scan demonstrated significantly dilated small bowel loops with mesenteric congestion, supporting the diagnosis of small bowel obstruction, though a clear transition zone was not identified [Fig.1a].
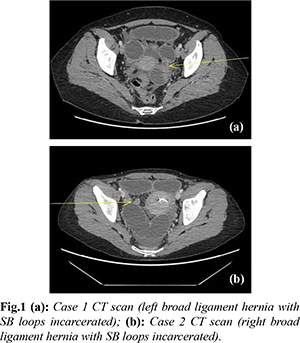
Initial management involved intravenous fluid resuscitation, nasogastric tube placement, and urinary catheterization. After 11 hours, she underwent emergency theatre following NCEPOD (National Confidential Enquiry into Patient Outcome and Death) protocols. Diagnostic laparoscopy revealed small bowel obstruction due to an internal hernia within the right broad ligament [Fig.1a]. The herniated bowel segment was congested but viable, allowing for careful reduction and inspection. Closure of the broad ligament defect was achieved with a V-lock suture [Fig.2]. The post-operative period was uneventful, and she was discharged on the second operative day.
Case 2
A 47-year-old woman presented to the medical team with a 3-day history of abdominal pain radiating from the pubic region to umbilicus. She experienced bilious vomiting, constipation, and reported coffee-brown vomitus. With a past medical history of hiatus hernia and reflux oesophagitis, she displayed a distended abdomen with tenderness over the umbilical region. Initial clinical observations, including a saturation of 96% on 2L, temperature of 37°C, BP 140/88 mm Hg, and RR 18/min, indicated ASA 2 status. On admission, a CRP of 35 mg/L was noted with otherwise unremarkable values (WBC 7x109/L and normal lactate). Plain abdominal X-ray revealed a few dilated loops of small bowel in the mid abdomen. Treatment for small bowel obstruction commenced, involving nil orally, intravenous fluids, nasogastric tube insertion, and catheterization, along with proton pump inhibitors and intravenous antibiotics. The patient was promptly referred to the surgical team, and a subsequent CT scan revealed small bowel obstruction originating in the pelvis with a transition zone in the left hemi-pelvis and minimal ascites [Fig.1b].
NCEPOD emergency laparoscopy, performed 11 hours after admission, uncovered dilated and collapsed small bowel loops herniating through a defect in the left broad ligament [Fig.3]. The small bowel was gently reduced, and the defect was closed using laparoscopic clips. The recovery was uneventful, and the patient was discharged on the second post-operative day.
Discussion
Despite the rarity of broad ligament hernias, their presentation is often acute and characterized by small bowel obstruction. Timely diagnosis is paramount for effective management, with contrast-enhanced abdominal CT scans serving as the cornerstone of diagnostic assessment [2]. CT scans typically reveal pelvic small bowel obstruction with dilated loops, fluid levels, potential closed loop obstruction, and serous fluid accumulation in the pelvis. While small bowel herniation with incarceration is the most common complication, other viscera such as ovaries and ureters may also be involved. Surgical intervention for broad ligament hernias entails the gentle reduction of incarcerated small bowel loops and contents in the Trendelenburg position, followed by the repair of the hernia defect using clips or sutures. While a laparotomy is often the standard surgical approach, laparoscopic exploration and repair can be safely executed when ischemic small bowel obstruction is ruled out.
Broad ligament hernias are classified into two types based on nature and anatomy, as detailed in Table 1 [8,9]. The classification system proposed by Hunt and Cilley provides a valuable framework for understanding the diverse manifestations of broad ligament hernias. This classification recognizes the intricate variations in hernia presentation and highlights the importance of individualized treatment approaches for optimal patient outcomes. As our understanding of these hernias evolves, this classification system serves as a cornerstone for refining diagnostic and therapeutic paradigms in the realm of acute broad ligament hernias.
The diagnostic utility of contrast-enhanced abdominal CT scans in the context of acute broad ligament hernias cannot be overstated. These imaging studies not only contribute to the confirmation of small bowel obstruction but also offer critical insights into the specific characteristics of the hernia, including the location and extent of the defect. The identification of these features guides surgical planning, allowing for a targeted and effective approach during the intervention. Furthermore, the comprehensive nature of CT scans aids in the assessment of potential complications such as closed loop obstruction, which may influence the choice of surgical technique and post-operative management.
The two cases presented with acute small bowel obstruction, clinically diagnosed and radiologically confirmed through CT scans. Initial management included fluid resuscitation and small bowel decompression with a nasogastric tube. Surgical intervention via diagnostic laparoscopy provided clear visualization of the incarcerated small bowel within the broad ligament defect. Following the reduction of the small bowel, improved viability facilitated the laparoscopic closure of the broad ligament defect.
Conclusion
These cases highlight the significance of a multidisciplinary approach in effectively managing acute broad ligament hernias and highlights the potential role of laparoscopic techniques in appropriate cases.
Contributors: CM: manuscript writing, patient management; MAG: manuscript editing, patient management. CM will act as a study guarantor. Both authors approved the final version of this manuscript and are responsible for all aspects of this study.
Funding: None; Competing interests: None stated.
References
- Griffiths S, Glancy D. Intestinal obstruction. Intestinal Surgery. 2020;38(1):43-50.
- Lanzetta M, Masserelli A, Addeo G, Cozzi D, Maggialetti N, Danti G, et al. Internal hernias: a difficult diagnostic challenge. Review of CT signs and clinical findings. Acta Biomed. 2019;24:20-37.
- Quain R. Case of internal strangulation of a large portion of the ileum. Trans Path Soc Lond. 1861;12:103-104.
- Murali Appavoo Reddy U, Dev B, Santosham R. Internal hernias: Surgeons dilemma-unravelled by imaging. Indian J Surg. 2014;76(4):323-328.
- Welch C. Hernia: intestinal obstruction. Chicago: Year Book Medical. 1958;239-268.
- Zemour J, Coueffe X, Fagot H. Herniation of the broad ligament. And the other side? Int J Surg Case Rep. 2019(65):354-357.
- Varela G, López-Loredo A, García León J. Broad ligament hernia-associated bowel obstruction. JSLS 2007;11(1):127-130.
- Cilley R, Poterack K, Lemmer J, Dafoe D. Defects of the broad ligament of the uterus. Am J Gastroenterol. 1986;81:389-391.
- Hunt A. Fenestra and pouches in the broad ligament as an actual and potential cause of strangulated intraabdominal hernia. surgery. Gynecology, Obstetrics. 1934;58:906-913.