|
|
|
|
|
Cancer Related Atypical Hemolytic Uremic Syndrome with Cepacia Syndrome
|
|
|
|
Sneha Manesh, Preethi N, K Jyoshna Devi, Rathnasree D Department of Clinical Pharmacy Practice, Samskruti College of Pharmacy, Jawaharlal Nehru Technological University, Hyderabad, Telangana, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr Sneha Manesh Email: snehamanesh1915@gmail.com |
|
|
|
|
|
|
|
|
Received:
06-FEB-2024 |
Accepted:
18-APR-2024 |
Published Online:
15-JUL-2024 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: Cancer related hemolytic uremic syndrome (C-HUS) with Cepacia syndrome is a medical emergency and is a serious complication of metastatic cancer that needs immediate medical intervention. This report is of a woman who is a known case of adenocarcinoma of stomach stage 4 with liver metastasis, and Cepacia syndrome. Case Report: A 61-year-old female patient, known case of stage 4 carcinoma of stomach with liver metastasis who is post second line treatment on palliative chemotherapy presented to the department of oncology with complaints of progressive shortness of breath, weakness, abdominal pain and pedal edema. All the necessary investigations were done. Blood culture and sensitivity report indicated Burkholderia cepacia infection. Complete blood picture revealed presence of schistocytes and toxic neutrophils. Supportive care and symptomatic relief were provided to the patient. Conclusion: This case highlights an atypical presentation of C-HUS with Cepacia syndrome and challenges of managing HUS in immunocompromised cancer patients. |
|
|
|
|
|
Keywords :
|
Burkholderia cepacia, Carcinoma, Hemolytic Anemia, Hemolytic Uremic Syndrome, Metastasis, Thrombotic Microangiopathies.
|
|
|
|
|
|
|
|
|
|
|
|
Introduction
The trio of hemolytic anemia (hemoglobin < 10 g/dL) with fragmented erythrocytes (schistocytes), thrombocytopenia (platelets < 1,50,000/mm 3), and renal impairment (serum creatinine > upper limit of normal for age) characterize HUS. Non-immune hemolysis is defined by a negative Coomb’s test, except for false positivity in S. pneumoniae HUS. Endogenous haptoglobin is undetectable and elevated lactate dehydrogenase (LDH) levels support intravascular hemolysis. Microangiopathic anemia is the underlying histological lesion, characterized by thickening of capillary and arteriole walls, severe endothelial damage (swelling and dislocation), and sub-endothelial buildup of fibrin, proteins, and cell debris platelet rich thrombi blocking the lumina of the vessel. Microangiopathic thrombotic anemia impacts renal microvasculature primarily. While the heart, brain, lungs and gastrointestinal system could have a role [ 1], infectious diarrhea primarily caused by Escherichia coli O157:H7 or Shiga toxin-producing Escherichia coli (STEC) is the most frequent predisposing factor leading to typical HUS. On the other hand, there are other potential causes of HUS such as cancer, pregnancy, organ transplantation, HIV, upper respiratory tract infections, non-E. coli diarrheal diseases, and the use of certain medications like oral tacrolimus, quinine, cyclosporine, ticlopidine and oral contraceptives (OCPs). Atypical HUS makes up about 5-10% of all recorded instances of HUS and is linked to poor prognosis [ 2]. Cancer related hemolytic uremic syndrome (C-HUS) is distinguishable from disorders such as thrombotic thrombocytopenic purpura, consuming coagulopathy, infantile HUS and microangiopathic hemolysis linked to advanced cancer. There is a 4-5% chance of developing C-HUS following treatment with chemotherapeutic agents such as mitomycin, oxaliplatin, gemcitabine and irinotecan [ 3, 4]. Recommendations include monitoring of all patients having C-HUS for changes in their hematologic and renal functions; patients suspected of having C-HUS should have vigorous non-transfusion on the other hand, patients with definite syndrome should be advised SPA immunopheresis treatment [ 5]. Since cancer patients are immunocompromised, they tend to develop opportunistic infections which can be life threatening. Burkholderia cepacia is a gram-negative bacteria known to cause high incidence of morbidity and mortality in immunocompromised patients. Insufficient data collection and no accurate laboratory data have resulted in scarcity of accurate reports of Burkholderia infection incidence and prevalence in India. These bacteria have been dubiously identified as pseudomonas species in most cases. Only a few percent of tertiary care facilities in North India have reported cases [ 6]. Inhaled or parenteral antibiotics, alone or in combination with corticosteroids are required for the management. It is crucial to decide the dosage, combination and duration of treatment beforehand [ 7].
Case Report
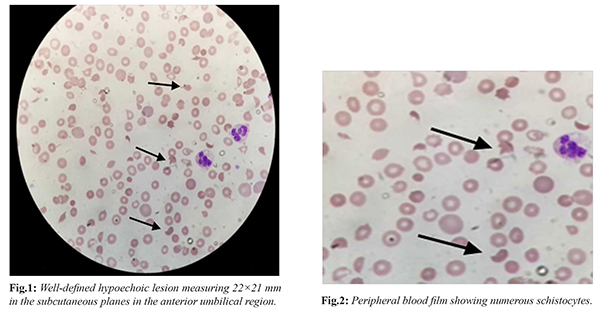
A 61-year-old female patient, known case of stage 4 carcinoma of stomach with liver metastasis who is post second line treatment on palliative chemotherapy presented to the department of oncology with complaints of progressive shortness of breath for last 3 days, weakness, abdominal pain for last 4 days and pedal edema for 15 days (about 2 weeks). On clinical examination, the patient was found to have anasarca, mild pallor, dense ascites and bilateral pleural effusion which was etiologically related to hypoproteinemia. Vitals on admission were found to be blood pressure: 130/80 mmHg, pulse rate: 122/min, SPO2: 98% on room air. She has a history of diabetes, hypertension and hypothyroidism on regular medications. Upper gastrointestinal (UGI) endoscope could not be negotiated beyond 35 cm (about 1.15 ft). The necessity of feeding through jejunostomy for nutritional support was explained to the patient and family members but they opted out. She received total parental nutrition (TPN) and albumin twice to maintain the nutrition. During the hospital stay, she had complaints of hematuria, serum creatinine was found to be increased by 1.5 mg/dL which indicated acute kidney injury (AKI). History of chemotherapy with FOLFOX regimen, completed 11 cycles later she was on 2 cycles of XELIRI regimen. Patient received last cycle 5 months ago. On worsening of symptoms, patient was shifted to the department of critical, patient was found to have sepsis, platelet levels dropped to 18,000/cu.mm. Furthermore, laboratory investigations were carried out. Hematological examination revealed hemoglobin of 10.5 g/dL (reference range: 12-15 g/dL), white blood cell count 10,630/cu.mm (reference range: 4000-10,000/cu.mm), red blood cell count 3.65 million/cu.mm (reference range 4.3-4.8 million/cu.mm), hematocrit of 31.7% (reference range: 35-45%), red cell distribution width 22.8% (reference range 12-17%), and platelet count of 30,000/cu.mm (reference range: 1.5-4.5L). Numerous schistocytes were observed, neutrophils exhibited toxic granules within cytoplasmic vacuoles, and a few large platelets were noted [Fig.1,2]. The urine culture and sensitivity report revealed Extended Spectrum Beta Lactamase (ESBL) Escherichia coli with a colony count of >105Cfu/mL susceptible to Piperacillin/Tazobactam. The blood culture and sensitivity test stated the presence of Burkholderia cepacia susceptible to ciprofloxacin and meropenem. Coombs test was found to be negative. Biochemistry report revealed lactate dehydrogenase levels to be 449 IU/L (reference range 0-330 IU/L), high sensitivity troponin I levels were found to be 136.80 pg/mL (reference range 0-19.80 pg/mL), C-reactive protein (CRP) levels were found to be 12 mg/L (reference range <6 negative, 6 and above positive). Renal function test revealed urea levels to be 60 mg/dL (reference range 15-45 mg/dL), creatinine levels were found to be 2 mg/dL (reference range 0.5-1.2 mg/dL), sodium 134 mmol/L (reference range 138-145 mmol/L). The liver function test revealed total protein levels to be 3.4 g/dL (reference range 6.4-8.3 g/dL), albumin 2.2 g/dL (reference range 3.8-5.4 g/dL), total bilirubin levels were found to be 1.5 mg/dL (reference range 0.1-1.2 mg/dL), unconjugated bilirubin levels were found to be 1.7 mg/dL (reference range 0.2-1.2 mg/dL), SGOT, SGPT and ALP levels were found to be normal. Chest X-ray report revealed chemo port in situ, mild haziness noted in right lung parenchyma and bilateral pleural effusion left > right. ECG indicated T wave abnormalities. 2D ECHO report showed tachycardia, no regional wall motion abnormality (RWMA), fair left ventricular systolic function, normal sized chamber with mild mitral regurgitation. As per the investigations, the patient was diagnosed with hemolytic uremic syndrome which was etiologically cancer related due to underlying adenocarcinoma of stomach. During nine days of hospital stay, the patient received supportive care in the form of intravenous fluids, antibiotics, one single donor platelet for thrombocytopenia, large volume paracentesis was done under albumin cover, bilateral pleural tapping was done twice to improve her shortness of breath and symptomatic relief was provided to the patient. She was off oxygen support, maintained SpO2 of 99% on room air and blood pressure at the time of discharge was of 100/60 mmHg, on TPN with resolving AKI and urinary tract infection but schistocytes and thrombocytopenia were found to be persistent. The patient developed hypokalemia and was treated with potassium chloride with magnesium sulphate. The patient and the family members were counselled regarding the patient’s condition and prognosis and were motivated for best supportive care at home.
Discussion
The most prevalent form of thrombotic microangiopathy (TMA), hemolytic uremic syndrome (HUS) is characterized by acute kidney injury, thrombocytopenia and microangiopathic hemolytic anemia (MAHA). TMA can occur due to cancer or chemotherapy. The underlying mechanism of cancer associated TMA is etiologically associated to systemic microvascular metastases and bone marrow metastases or necrosis whereas the underlying mechanism of chemotherapy induced TMA is etiologically associated to dose dependent toxicity and drug dependent antibody reaction. TMA are divided into three main groups: thrombotic thrombocytopenic purpura (TTP), atypical HUS (a-HUS) and Shiga toxin producing Escherichia coli hemolytic uremic syndrome (STEC-HUS) [8]. HUS can be cancer related or chemotherapy induced. a-HUS cause an over-activation of the complement pathway and variety of etiologies, including hereditary and acquired. Due to misdiagnosis or late diagnosis it leads to higher incidence of mortality. It is characterized by the presence of schistocytes. Reticulocytosis, elevated lactate dehydrogenase (LDH), low or non-existent haptoglobin, and elevated unconjugated bilirubin levels are additional indicators of hemolysis. While treating cancer associated or chemotherapy induced C-HUS, it is important to identify the underlying cause of the illness (the drug or the cancer) and prevent unnecessary treatments like plasma exchange to avoid complications [ 9]. When evaluating cancer patients for HUS chemotherapy treatment, other co-morbidities and their undergoing treatment must be considered then the offending agent must be stopped immediately. Prolonged exposure to chemotherapeutic agents also could possibly lead to HUS. Cancer patients undertake several cycles of chemotherapy which compromises their immune system, Due to this there rises a high risk of opportunistic infections. Cepacia syndrome is characterized by pneumonia with significant radiologic changes, multi organ damage and bacteremia [ 10]. The treatment options mainly include fluoroquinolones, carbapenems and 4th generation cephalosporins.
Conclusion
In this case, a 61-year-old female with stage 4 gastric carcinoma and liver metastasis developed hemolytic uremic syndrome (HUS), characterized by acute kidney injury, thrombocytopenia, and microangiopathic hemolytic anemia. Despite receiving antibiotics, supportive care, and symptomatic relief, her condition was complicated by opportunistic infections, highlighting the challenges of managing HUS in immunocompromised cancer patients. Early diagnosis, regular monitoring, and differentiation between chemotherapy-induced and cancer-associated HUS are crucial for effective treatment and improved patient outcomes.
Contributors: SM: manuscript writing, literature search; PN, KJD: manuscript editing and literature search; RD: critical inputs into the manuscript. SM will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study. Funding: None; Competing interests: None stated.
References - Loirat C, Frémeaux-Bacchi V. Atypical hemolytic uremic syndrome. Orphanet J Rare Dis. 2011;6;60.
- Sethi A, Moses R. Atypical hemolytic uremic syndrome: Cancer-induced or chemotherapy-induced? Cureus. 2021;21(2):e13260.
- Lesesne JB, Rothschild N, Erickson B, Korec S, Sisk R, Keller J, et al. Cancer-associated hemolytic-uremic syndrome: analysis of 85 cases from a national registry. J Clin Oncol. 1989;7(6):781-789.
- Aklilu AM, Shirali AC. Chemotherapy-associated thrombotic microangiopathy. Kidney360. 2023;4(3):409-422.
- Garibotto G, Acquarone N, Saffioti S, Deferrari G, Villaggio B, Ferrario F. Successful treatment of mitomycin C-associated hemolytic uremic syndrome by plasmapheresis. Nephron. 1989;51(3):409-412.
- Sapkota S, Ganesan S, Bhattacharjee S, Priyadarshini M, Tripathi P, ShobaSavitha A, et al. Clinical spectrum of Burkholderiacepaciainfection in cancer patients: A retrospective study of an emerging disease. Med Microbiol Rep. 2019;2:1-4.
- Ottu Para NK, Vemuri S, Koshy G, Ibrahim D, Oomen S, Reddappa SV, et al. Management of Cepacia syndrome in an immunocompetent non-cystic fibrosis adult patient. Int J Infect Dis. 2022;122:550-552.
- Barbour T, Johnson S, Cohney S, Hughes P. Thrombotic microangiopathy and associated renal disorders. Nephrology Dialysis Transplantation. 2012;27(7):2673-2685.
- Thomas MR, Scully M. How I treat microangiopathic hemolytic anemia in patients with cancer. Blood. 2021;137(10):1310-1317.
- Loutet SA, Valvano MA. A decade of Burkholderia cenocepacia virulence determinant research. Infect Immun. 2010;78(10):4088-4100.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Manesh S, Preethi N, Devi KJ, Rathnasree DCancer Related Atypical Hemolytic Uremic Syndrome with Cepacia Syndrome.JCR 2024;14:57-60 |
|
Manesh S, Preethi N, Devi KJ, Rathnasree DCancer Related Atypical Hemolytic Uremic Syndrome with Cepacia Syndrome.JCR [serial online] 2024[cited 2026 May 8];14:57-60. Available from: http://www.casereports.in/articles/14/3/Cancer-Related-Atypical-Hemolytic-Uremic-Syndrome-with-Cepacia-Syndrome.html |

|
|
|
|
|