|
|
|
|
|
Dermatofibrosarcoma Protuberans: A Rare Metastasis to Pancreas
|
|
|
|
Himangsu Sarma, Hariharan Ramesh, John M Madipadam, Iona Leekha Mathew Department of Surgical Gastroenterology, Lakeshore Hospital and Research Centre, Kochi, Ernakulam, Kerala, India 682040. |
|
|
|
|
|
Corresponding Author:
|
|
Dr Himangsu Sarma Email: himangsu59@gmail.com |
|
|
|
|
|
|
|
|
Received:
17-NOV-2024 |
Accepted:
02-APR-2025 |
Published Online:
05-AUG-2025 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: Dermatofibrosarcoma protuberans (DFSP) is a rare, slow-growing, locally aggressive soft tissue malignancy. While it carries a high risk of local recurrence, its metastatic potential is low. Metastasis to the pancreas is extremely uncommon, with only a handful of cases reported in the literature. Case Report: We describe the case of a 34-year-old woman with DFSP of the right breast who underwent multiple surgeries between 2014 and 2019. During follow-up in 2021, she developed abdominal pain, and imaging revealed a pancreatic mass. Tru-cut biopsy confirmed metastatic DFSP. She subsequently underwent two major resections in 2021, including en-bloc tumor excision and distal pancreato-splenectomy. In 2024, she developed recurrence from the resected pancreatic margin and underwent further tumor debulking. Despite receiving multiple lines of tyrosine kinase inhibitors and chemotherapy, her disease course was marked by repeated recurrences. Conclusion: Although DFSP is primarily a locally aggressive tumor with low metastatic potential, rare systemic metastases, including to the pancreas, can occur. This case highlights the importance of considering metastatic DFSP in unusual locations and emphasizes the need for long-term follow-up and multidisciplinary management. |
|
|
|
|
|
Keywords :
|
Abdominal Pain, Breast, Chemotherapy, Excision, Metastases.
|
|
|
|
|
|
|
|
|
|
|
|
Introduction
Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive dermal tumor of fibroblastic origin that arises from the subcutaneous mesenchymal tissue of the skin. It is characterized by high rates of local recurrence but only infrequent systemic metastasis. DFSP most commonly involves the trunk and proximal extremities and typically affects individuals between 20 and 50 years of age [ 1, 2]. A chromosomal translocation, t(17;22), has been identified in approximately 90% of cases [ 2]. Metastatic spread to the pancreas is extremely uncommon, with only a few cases documented in the literature. Management of metastatic disease usually involves surgical resection combined with adjuvant therapy using tyrosine kinase inhibitors.
Case Report
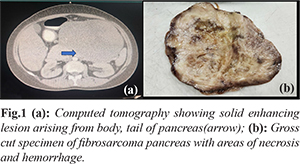
A 34-year-old woman, previously diagnosed with dermatofibrosarcoma protuberans (DFSP) of the right breast, underwent lumpectomy in 2014 followed by six cycles of adjuvant chemotherapy (idarubicin and cytarabine) and one year of imatinib. Despite therapy, she experienced local recurrence requiring multiple breast surgeries up to 2019. In 2021, during evaluation for abdominal pain, contrast-enhanced computed tomography (CECT) revealed an 18×15 cm solid enhancing mass arising from the body and tail of the pancreas, abutting the posterior serosa of the antro-pyloric region of the stomach [Fig.1a]. Tru-cut biopsy demonstrated a spindle cell neoplasm with a Ki-67 index of 29%. Clinically, a hard mass was palpable in the left hypochondrium and epigastrium, extending below the umbilicus. The patient underwent laparotomy with complete excision of the intra-abdominal tumor in May 2021. No distant metastases were observed intraoperatively. Histopathology confirmed DFSP (FNCLCC Grade 2). A follow-up CECT in August 2021 demonstrated a well-defined 4×3 cm lobulated lesion arising from the mid-body of the pancreas with enhancing nodular areas and associated splenic vein thrombosis. Positron emission tomography (PET)-CT revealed recurrent disease in the pancreatic body (5×3 cm) with nodular necrosis. Endoscopic ultrasound (EUS)-guided fine-needle cytology again suggested a spindle cell tumor. In October 2021, she underwent open distal pancreato-splenectomy. Intraoperatively, a 5×5 cm well-defined tumor was identified in the body of the pancreas, adherent to the mesocolon and posterior gastric wall [Fig.1b]. Pathology showed pT2N0 disease.
She was initiated on pazopanib, a tyrosine kinase inhibitor, in place of imatinib, and therapy was continued until March 2024. At that time, she presented with recurrent abdominal pain of three weeks’ duration. Repeat CECT demonstrated a 15×9 cm mass at the resection margin of the pancreas, with multiple metastatic deposits involving the bilateral adnexa, pancreatic head and uncinate process, greater curvature of the stomach, and retroperitoneum [Fig.2]. Debulking surgery was performed. Microscopic examination revealed neoplastic spindle cells arranged in storiform and whorled patterns, with focal necrosis and areas resembling a herringbone architecture [Fig.3]. Immunohistochemistry (IHC) demonstrated positivity for vimentin and weak CD34 expression in fibrosarcomatous areas, while S100, STAT6, SMA, desmin, CD117, and beta-catenin were negative [Fig.4]. The patient is currently under close follow-up in the oncology outpatient clinic and is being treated with axitinib, a tyrosine kinase inhibitor.
Discussion
Dermatofibrosarcoma protuberans (DFSP) was first described by Darier and Ferrand in 1924 [ 1]. It originates from fibroblasts in the subcutaneous mesenchymal tissue of the skin and most commonly involves the trunk (50%) and proximal extremities (20%-35%). The peak incidence is between 20 and 50 years of age. Metastasis to the pancreas is exceedingly rare, with the first reported case described by Atucha in 1960 [ 1]. Overall, 80%-90% of DFSP cases are associated with a high rate of local recurrence (26%) but relatively low risk of distant metastasis (5%). Cytogenetic studies have shown that the majority harbor a t(17;22)(q22;q13) translocation, resulting in fusion of the COL1A1 and platelet-derived growth factor B (PDGFB) genes. This leads to PDGFB overexpression and is seen in approximately 90% of DFSP cases [ 2]. In early stages, patients are usually asymptomatic. As the tumor enlarges, symptoms may arise due to compression of adjacent structures, including gastrointestinal obstruction, jaundice, abdominal pain, or cachexia [1]. Diagnosis is typically established with CT or MRI. On MRI, DFSP lesions often appear hypointense on T1-weighted images and slightly hyperintense on T2-weighted images, with a characteristic spoke wheel-like enhancement [1]. The differential diagnosis includes non-functional islet cell tumors, solid pseudopapillary neoplasms, pancreatic carcinoma, and other rare pancreatic tumors [2]. Definitive diagnosis requires histopathology and immunohistochemistry (IHC). Biopsy generally reveals diffusely distributed spindle cells interwoven with matrix elements and abundant vasculature [1]. Fibrosarcomatous areas display a herringbone architecture and high mitotic activity. IHC typically shows positivity for vimentin and platelet-derived growth factor receptor (PDGFR), diminished or absent CD34 expression, and negativity for S100, SMA, and CD117 [1,2]. The cornerstone of treatment is wide local excision with tumor-free margins, which significantly reduces the risk of recurrence [3]. For solitary resectable tumors, surgical resection may be curative. Metastatic DFSP is challenging to treat, as fibrosarcomatous variants are often resistant to conventional chemotherapy [1]. Tyrosine kinase inhibitors (TKIs) such as imatinib have shown significant efficacy in metastatic, locally advanced, unresectable, or disseminated DFSP harboring the t(17;22) translocation [4]. Other TKIs, including sunitinib, pazopanib, and axitinib, have also demonstrated clinical activity. Radiotherapy (50–60 Gy) is considered in patients with margin-positive resections, large unresectable tumors, or multiple recurrences [5]. In our case, the patient achieved a median progression-free survival of nearly two years with systemic therapy. However, outcomes were poor following disease progression on imatinib, highlighting the need for more effective second-line options.
Conclusion
DFSP is a malignancy of low metastatic potential, its propensity for local recurrence emphasizes the importance of preoperative imaging, meticulous surgical planning, and close postoperative surveillance. Wide local excision remains the mainstay of treatment. Advanced or metastatic cases require a multidisciplinary approach, with tyrosine kinase inhibitors, particularly imatinib, forming the cornerstone of systemic therapy. Second-line agents such as pazopanib and axitinib may provide temporary benefit, but evidence is limited to anecdotal reports. Continued research and clinical experience are essential to improve management strategies for this rare entity.
Contributors: HS: manuscript writing and concept; HR: manuscript editing; JMM, ILM: critical inputs into the manuscript. HS will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study. Funding: None; Competing interests: None stated.
References - Cai HJ, Fang JH, Cao N, Wang W, Kong FL, Sun XX, et al. Dermatofibrosarcoma metastases to the pancreas: A case report. World J Clin Cases. 2019;7(20):3316-3321.
- Chilukuri DS, Premkumar P, Venkitaraman B, Soundararajan JCB. Pancreatic metastasis of dermatofibrosarcoma protuberans: a rare case. BMJ Case Rep. 2020;13(1):e232614.
- Murata H, Ohashi A, Ashida A, Uhara H, Okuyama R, Nakata T, et al. Fibrosarcomatous variant of dermatofibrosarcoma protuberans with pancreatic metastasis. Int J Dermatol. 2014;53(2):e140-142.
- Labropoulos SV, Razis ED. Imatinib in the treatment of dermatofibrosarcoma protuberans. Biologics. 2007;1(4):347-353.
- Noujaim J, Thway K, Fisher C, Jones RL. Dermatofibrosarcoma protuberans: from translocation to targeted therapy. Cancer Biol Med. 2015;12(4):375-384.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Sarma H, Ramesh H, Madipadam JM, Mathew I LDermatofibrosarcoma Protuberans: A Rare Metastasis to Pancreas.JCR 2025;15:57-60 |
|
Sarma H, Ramesh H, Madipadam JM, Mathew I LDermatofibrosarcoma Protuberans: A Rare Metastasis to Pancreas.JCR [serial online] 2025[cited 2026 Jun 4];15:57-60. Available from: https://www.casereports.in/articles/15/3/Dermatofibrosarcoma-Protuberans.html |

|
|
|
|
|