|
|
|
|
|
World’s Largest Neglected Parosteal Lipoma Presenting as Deep Vein Thrombosis of the Lower Limb: An Extremely Rare Presentation
|
|
|
|
Islam S1,2, Ramoutar K1, Bheem V1, Harnarayan P1,2, Naraynsingh V2 1Consultant General, Laparoscopic and Oncoplastic Breast Surgery, San Fernando Teaching Hospital and 2Department of Clinical Surgical Sciences, University of the West Indies, St Augustine, Trinidad and Tobago. |
|
|
|
|
|
Corresponding Author:
|
|
Dr Shariful Islam Email: sssl201198@yahoo.com |
|
|
|
|
|
|
|
|
Received:
02-SEP-2024 |
Accepted:
06-MAY-2025 |
Published Online:
25-AUG-2025 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: Parosteal lipomas are rare benign tumors of adipose tissue located on the cortical surface of bone. They represent only a small fraction of bone lipomas, and most reported cases are small and incidentally detected. Presentation with deep vein thrombosis (DVT) has not been described previously. Case Report: We present a 61-year-old male with acute right lower limb pain diagnosed as popliteal vein DVT. Evaluation revealed a giant 30 cm parosteal lipoma of the femur, the largest reported to date. The lesion was completely excised, and the patient made an uneventful recovery with no recurrence on long-term follow-up. Conclusion: This case describes to best of our knowledge the world’s largest parosteal lipoma and its unusual presentation with DVT. Complete surgical excision through a multidisciplinary approach is essential for cure and to prevent recurrence. |
|
|
|
|
|
Keywords :
|
Adipose Tissue, Benign Tumor, Bone, Femur, Lipoma, Pain.
|
|
|
|
|
|
|
|
|
|
|
|
Introduction
Bone lipomas are uncommon lesions, usually asymptomatic, and may occur either as juxta-cortical (arising on the bone surface) or intra-osseous (originating within the bone) variants. Among juxta-cortical types, sub-parosteal and parosteal forms are described [ 1, 2]. Parosteal lipomas are extremely rare benign tumors of adipose tissue, generally asymptomatic and often overlooked, most frequently affecting individuals in middle age. They tend to arise as solitary lesions in the extremities, with the tibia, femur, radius, and humerus being the most common sites of occurrence [ 3- 6]. These tumors are characteristically associated with the periosteum and may occasionally produce periosteal changes [ 7]. To the best of our knowledge, we present the case of the world’s largest parosteal lipoma of the femur in a 61-year-old male, who manifested with deep vein thrombosis but without periosteal changes or neural involvement
Case Report
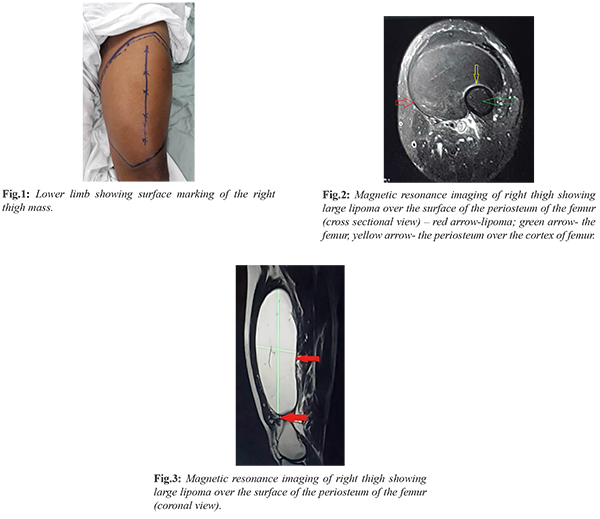
A 61-year-old male, known diabetic and hypertensive, presented to the Accident and Emergency Department with acute right lower limb pain for the past 24 hours. He reported a swelling in the right thigh for the last four years, which had initially remained the size of an apple but had shown rapid enlargement during the past year. There was no history of trauma. His past medical history included a right hip replacement and brachytherapy for prostate cancer around ten years earlier. A Doppler ultrasound confirmed deep vein thrombosis of the right popliteal vein, and the patient was admitted under the medical team. Thrombophilia screening was negative, and he was started on therapeutic clexane before being referred to the on-call surgical team. On examination, the right thigh was diffusely swollen, and a large 30×25 cm soft-to-firm, elliptical mass with a smooth surface and slight mobility was palpable [Fig.1]. The overlying skin was normal, and no inguinal lymphadenopathy was noted. Peripheral pulses and sensations were intact. Radiography revealed a radiolucent lesion with no evidence of fractures or bony involvement, while MRI demonstrated a 30×13×10.5 cm well-defined, high-intensity lesion deep in the anterior compartment musculature but located on the surface of the femoral shaft. The lesion did not involve the underlying bone or adjacent vascular structures [Fig.2,3]. A true-cut biopsy revealed skeletal muscle, fibro-adipose tissue, and scattered mononuclear cells, with no evidence of malignancy.
Following multidisciplinary team discussion, the patient was planned for surgical excision. Under general anesthesia and in the supine position, a vertical incision was made over the anterior thigh. The skin, subcutaneous tissue, and rectus femoris muscle were retracted to expose the mass [Fig.4], which was then carefully dissected and excised in its entirety from the surface of the femoral shaft along with periosteum [Fig.5,6]. Postoperatively, the patient developed transient weakness of the right lower limb, which improved with physiotherapy. There was no sensory loss, and he was mobilized and discharged on warfarin for three months. At three-month follow-up, a repeat duplex scan confirmed recanalization of the deep vein, and anticoagulation was discontinued. Histopathological examination reconfirmed the diagnosis of parosteal lipoma [Fig.7]. The patient remained well during subsequent follow-up and was discharged from the surgical clinic at six months. A telephone follow-up conducted almost four years after surgery confirmed that he remained asymptomatic, with no recurrence or new complaints.
Discussion
Parosteal lipomas, first described by Power in 1888, are rare benign tumors of adipose tissue that arise directly on the cortex of bone [ 1]. The WHO defines a bone lipoma as a benign neoplasm of adipose tissue that may occur within the medullary cavity, the cortex, or on the bone surface [ 2]. Histologically, they resemble the more common soft tissue lipomas and are believed to originate from mesenchymal cells of the periosteum. These tumors are extremely uncommon, accounting for only 0.3% of all lipomas and 0.1% of all primary bony tumors [ 3, 5]. Based on their morphology, parosteal lipomas are divided into four types [4]. Type I lesions rest directly on the cortex without bone or cartilage elements, Type II lesions have a narrow bony stalk with a lipomatous cap resembling pedunculated exostosis, Type III contain a dense ossified osteo-chondromatous element beneath a lipomatous cap mimicking sessile exostosis, and Type IV contain patches of bone or cartilage scattered within the lipomatous tissue due to varying degrees of chondroid modulation or enchondral ossification. Our patient had no radiological or intraoperative evidence of bony involvement and therefore falls into the Type I category. Because these tumors are located deep within tissues, early diagnosis is often delayed, and they usually present only when they attain a large size or cause symptoms such as neuropathy [13]. The index case is unique in that the patient presented with deep vein thrombosis associated with a thigh mass, a feature not reported previously in the literature. Periosteal changes are observed in nearly 59.2% of cases, and it is essential to exclude malignancy in such situations [7]. For this reason, radiological and histopathological assessment is mandatory. Radiographs usually demonstrate a well-defined lucent mass adjacent to long bones, while CT further delineates the anatomy. However, MRI remains the most valuable imaging modality, as it accurately assesses the origin of the tumor from the periosteum and its relation to surrounding structures [14-16]. Histological confirmation by needle core or tru-cut biopsy should precede surgery in all suspected cases. Once malignancy has been excluded, the treatment plan depends on the presence of periosteal involvement. In cases without periosteal changes, simple surgical excision is considered curative, and recurrence has not been reported [5]. This was also observed in our patient, who remained disease-free over nearly five years of follow-up. However, when periosteal involvement is present, especially in deep tumors, the risk of malignancy is higher, and surgical planning requires a more cautious multidisciplinary approach, often involving plastic surgery support. Inadequate resection in such cases can result in recurrence or, rarely, malignant transformation [8]. Parosteal lipomas are usually located along the diaphysis of long bones, more commonly in females, with a mean age of presentation of 53 years (range 30-79 years). The most frequently affected sites include the femur, radius, tibia, and humerus [6-9]. Reported tumor sizes vary from a few centimetres to as large as 27 cm, with the average size being 7 cm. Very few cases exceeding 10 cm have been documented, and the largest case in literature to date was a recurrent 27 cm lesion reported by Soewoto W. et al. in 2022 [Table 1] [4,5,8-12]. The tumor in our patient measured 30 cm, making this the largest parosteal lipoma described worldwide to best of our knowledge.
Conclusion
Parosteal lipomas are rare, slow-growing, and usually benign tumors, but they may reach a very large size if neglected. Delays in diagnosis and treatment can result in compressive symptoms with significant morbidity. Any enlarging mass should undergo biopsy to rule out malignancy, and management should ideally be discussed in a multidisciplinary team setting. Complete surgical excision remains the treatment of choice and is essential to prevent recurrence. Giant parosteal lipomas should also be considered in the differential diagnosis of soft tissue sarcomas.
Contributors: IS, KR, AM, BV, HP and NV have contributed equally in drafting, writing, and critically analysing this article. IS will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study. Funding: None; Competing interests: None stated.
References - Power D. A parosteal lipoma, or congenital fatty tumor, connected with the periosteum of the femur. Tr Path Soc (London). 1888;39:270-272.
- Rosenberg AE BJ. Lipoma of bone. In: Fletcher CDM, Unni KK, Mertens F, editors. Pathology and genetics of tumors of the soft tissues and bones. Lyon: IARC Press; 2002. pp. 328-329.
- Grosch J. Studien uber das Lipom. Deutsche Ztschr Chir. 1887;26:307-382.
- Miller MD, Ragsdale BD, Sweet DE. Parosteal lipomas: a new perspective. Pathology. 1992;24:132-139.
- Fleming RJ, Alpert M, Garcia A. Parosteal lipoma. Am J Roentgenol. 1962;87:1075-1084.
- Elbardouni A, Kharmaz M, Berrada MS, Mahfoud M, Elyaacoubi M. Well- circumscribed deep-seated lipomas of the upper extremity. A report of 13 cases. 2011. J. Orthop Traumatol Surgery & Research. 2011; 2011(97):152-158.
- Aoki S, Kiyosawa T, Nakayama E, Inada C, Takabayashi Y, Sumi Y, et al. Large parosteal lipoma without periosteal changes. Plast Reconstr Surg Glob Open. 2015;3(1):e287.
- Soewoto W, Waskita B, Imamsoedjana AP. Case report: Recurrent parosteal lipoma at Dr. Moewardi hospital. Ann Med Surg (Lond). 2022;80:104061.
- Greco M, Mazzocchi M, Ribuffo D, Dessy LA, Scuderi N. Parosteal lipoma. Report of 15 new cases and a review of the literature. Ann Ital Chir. 2013;84(2):229-235.
- Jones JG, Habermann ET, Dorfman HD. Parosteal ossifying lipoma of femur. Skeletal Radiol.1989;18:537-540.
- Rodriguez-Peralto JL, Lopez-Barea F, Gonzalez-Lopez J, Lamas-Lorenzo M. Parosteal ossifying lipoma of femur. Skeletal Radiol. 1994;23:67-69.
- Bispo Junior RZ, Guedes AV. Parosteal lipoma of the femur with hyperostosis: case report and literature review. Clinics (Sao Paulo). 2007;62:647-652.
- Salama H, Kumar P, Bastawrous S. Posterior interosseous nerve palsy caused by parosteal lipoma: a case report. Case Rep Med. 2010:2010:785202
- Chaudhary RJ, Dube V, Bhansali C, Gupta A, Balwantkar S. Parosteal lipoma of humerus - a rare case. Int J Surg Case Rep. 2013;4:1159-1162.
- Murphey MD, Johnson DL, Bhatia PS, Neff JR, Rosenthal HG, Walker CW. Parosteal lipoma: MR imaging characteristics. Am J Roentgenol. 1994;162(1):105-110.
- Saksobhavivat N, Jaovisidha S, Sirikulchayanonta V, Nartthanarung A. Parosteal ossifying lipoma of the fibula: a case report with contrast-enhanced MR study and a review of the literature. Singapore Med J. 2012;53(8):e172-175.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Islam S, Ramoutar K, Bheem V, Harnarayan P, Naraynsingh VWorld’s Largest Neglected Parosteal Lipoma Presenting as Deep Vein Thrombosis of the Lower Limb: An Extremely Rare Presentation.JCR 2025;15:61-65 |
|
Islam S, Ramoutar K, Bheem V, Harnarayan P, Naraynsingh VWorld’s Largest Neglected Parosteal Lipoma Presenting as Deep Vein Thrombosis of the Lower Limb: An Extremely Rare Presentation.JCR [serial online] 2025[cited 2026 May 22];15:61-65. Available from: http://www.casereports.in/articles/15/3/Worlds-Largest-Neglected-Parosteal-Lipoma-Presenting-as-Deep-Vein-Thrombosis-of-the-Lower-Limb.html |

|
|
|
|
|