|
|
|
|
|
Metastatic Renal Cell Carcinoma to Small Bowel
|
|
|
|
Himangsu Sarma1, Hariharan Ramesh1, Vijaylakshmi Lekha1, Betcy Mary Babu2 Departments of 1Surgical Gastroenterology and 2Pathology, Lakeshore Hospital and Research Centre, Kochi, Ernakulam, Kerala-682040, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr Himangsu Sarma Email: himangsu59@gmail.com |
|
|
|
|
|
|
|
|
Received:
02-OCT-2025 |
Accepted:
09-FEB-2026 |
Published Online:
25-MAR-2026 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: Renal cell carcinoma (RCC) is the most common primary malignancy of the kidney and is known for its unpredictable metastatic behavior. Although it commonly spreads to the lungs, bones, liver, and brain, metastasis to the small intestine is extremely rare. Case Report: We report the case of a 47-year-old male with a known history of metastatic RCC who presented with symptoms of intestinal obstruction. Contrast-enhanced computed tomography (CECT) of the abdomen revealed dilatation and wall thickening of the distal jejunum along with an exophytic hypodense lesion in the upper pole of the right kidney. Due to persistent symptoms, the patient underwent diagnostic laparoscopy with resection and anastomosis of the obstructed proximal ileal segment. Histopathological examination of the resected bowel segment confirmed metastasis from RCC. The postoperative period was uneventful, and the patient was started on adjuvant systemic therapy with immunotherapy. Conclusion: Small bowel metastasis from RCC is rare and may present with intestinal obstruction. This case highlights the importance of considering metastatic disease in patients with a history of RCC presenting with gastrointestinal symptoms, as early recognition and appropriate management are essential for optimal patient care. |
|
|
|
|
|
Keywords :
|
Anastomosis, Bowel, Ileum, Metastasis, Obstruction, Renal Cell Carcinoma, Resection.
|
|
|
|
|
|
|
|
|
|
|
|
Introduction
Renal cell carcinoma (RCC) accounts for approximately 90% of all primary renal neoplasms and is most commonly observed in males during the fifth to sixth decade of life [ 1]. RCC is characterized by its unpredictable clinical course and its potential for distant metastasis. The most frequent sites of metastasis include the lungs, bones, liver, and brain, while involvement of the gastrointestinal tract is uncommon. Metastasis to the small intestine from RCC is extremely rare and only a limited number of cases have been reported in the literature. When it occurs, patients may present with nonspecific gastrointestinal symptoms such as abdominal pain, gastrointestinal bleeding, anemia, or intestinal obstruction, which can make diagnosis challenging. We report this rare case of metastatic RCC to the small bowel to highlight its unusual metastatic presentation and to increase clinical awareness of this uncommon site of metastasis in patients with a history of RCC presenting with gastrointestinal symptoms. Such case reports contribute to the limited available literature and may aid in earlier recognition and appropriate management of this rare condition [1].
Case Report
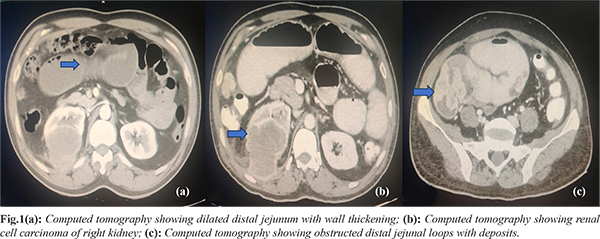
A 47-year-old male presented in 2023 with complaints of abdominal pain, vomiting, and constipation for seven days. He had a known history of clear cell type renal cell carcinoma (RCC) diagnosed in 2021 with metastases to the bone and right lung. At the time of diagnosis, he received palliative radiotherapy (30 Gy) to the thoracic vertebrae for bone metastasis. Subsequently, he was started on systemic therapy with pazopanib and axitinib. In September 2023, due to disease progression, a contrast-enhanced computed tomography (CECT) scan of the abdomen was performed. Imaging revealed an exophytic hypodense lesion measuring 5×4.9×5 cm in the upper pole of the right kidney along with dilatation and wall thickening of the distal jejunum and a few scattered omental deposits [Fig.1a]. At that time, the patient was receiving axitinib and denosumab. General physical examination was unremarkable. Abdominal examination revealed a distended abdomen with tenderness in the lower abdomen. An abdominal X-ray suggested sub-acute intestinal obstruction, and the patient was initially managed conservatively. However, due to persistent symptoms, a repeat CECT abdomen was performed, which showed similar findings along with newly identified mesenteric and jejunal deposits causing acute obstruction involving the distal jejunum [Fig.1b-c].
The patient subsequently underwent diagnostic laparoscopy with resection and anastomosis of the obstructed proximal ileal segment along with excision of omental deposits in October 2023. Intraoperatively, a large tumor measuring approximately 6×5 cm was identified involving the proximal ileum, causing near-complete obstruction. Gross examination of the resected ileal specimen measured 13.5 cm in length, and the mucosal surface showed three nodular lesions, the largest measuring 4×4×2 cm [Fig.2a-c]. On cut section, the lesion appeared grey-white and extended into the subserosa [Fig.3a]. Microscopic examination revealed an ulcerated neoplasm arranged in compact nests and sheets of tumor cells with intervening thin-walled vasculature. The tumor nests were separated by fibrous septae with associated lymphoplasmacytic infiltrate [Fig.3b-c]. Immunohistochemical analysis was consistent with metastatic RCC [Fig.3d-f]. The postoperative period was uneventful, and the patient was discharged in a stable condition. Following surgery, he continued systemic therapy with axitinib and adjuvant pembrolizumab for RCC. Follow-up CECT abdomen performed in March 2024 demonstrated further disease progression, and the patient is currently under ongoing management by the medical oncology team.
Discussion
Approximately 90% of all primary renal neoplasms are renal cell carcinomas (RCCs), with clear cell RCC representing the most common histological subtype, accounting for nearly 70% of cases [ 1]. RCC typically occurs between the ages of 50 and 70 years and is more frequently observed in males than females. RCC is well known for its ability to metastasize to distant organs. The most common sites of metastasis include the lungs, liver, brain, and lymph nodes, whereas involvement of the small intestine is extremely rare [ 1]. The first reported case of metastatic RCC to the small intestine was described in 1952 [ 2]. Metastasis of RCC to the small bowel may present with nonspecific gastrointestinal symptoms such as abdominal pain, gastrointestinal bleeding, anemia, or intestinal obstruction. Among these, intestinal obstruction is a significant complication. Contrast-enhanced computed tomography (CT) plays a crucial role in identifying intestinal obstruction and detecting metastatic lesions in the small bowel, thereby aiding in the diagnosis of metastatic RCC [3]. Histopathological examination along with immunohistochemistry (IHC) is essential for confirming the diagnosis. Tumor cells in metastatic RCC typically show positivity for markers such as Pan-CK (Pan-Cytokeratin), Vimentin, CD10, and epithelial membrane antigen (EMA), while being negative for CK7 and CK20 [4]. The immunohistochemical profile observed in our case was consistent with these findings and supported the diagnosis of metastatic RCC. Over the last two decades, an increase in the number of reported cases of small bowel metastasis from RCC has been observed. This rise may be attributed to advances in targeted therapies that have significantly improved the survival of patients with RCC [1]. Targeted agents such as bevacizumab, a vascular endothelial growth factor (VEGF) inhibitor, and immune checkpoint inhibitors such as pembrolizumab have contributed to improved disease control and prolonged survival. As a result, patients may live long enough to develop metastases at less common sites, including the small intestine [1]. In addition to surgical management, several systemic treatment options are available for metastatic RCC. Over the past 15 years, tyrosine kinase inhibitors (TKIs) have significantly transformed the management of metastatic RCC [5]. Agents such as sunitinib, sorafenib, and other second-line therapies have demonstrated improved survival outcomes in patients with metastatic disease [5]. Furthermore, newer therapies targeting the mammalian target of rapamycin (mTOR) signalling pathway and vascular endothelial growth factor receptors (VEGFR) have shown promising results. The combination of nivolumab (a PD-1 inhibitor) and ipilimumab (a CTLA-4 inhibitor) has also demonstrated improved overall survival and response rates compared with sunitinib in patients with intermediate- or poor-risk metastatic RCC [5]. In certain cases, small intestinal metastatic lesions may be unresectable or may present with complications such as acute intestinal obstruction or bleeding. In such situations, palliative procedures including enterostomy, bypass surgery, or urgent selective arterial embolization may provide symptomatic relief and improve the patient’s quality of life [5]. Recent updates from the European Association of Urology, the National Comprehensive Cancer Network (NCCN), and the American Urological Association (AUA) emphasize the importance of individualized surveillance strategies based on the patient’s risk profile and response to therapy, particularly during the first five years after treatment. However, long-term follow-up may also be necessary due to the possibility of late recurrence of RCC [5]. Therefore, small bowel metastasis should be considered as a potential cause in patients presenting with intestinal obstruction who have a prior history of renal cell carcinoma. Early recognition and appropriate management are essential to improve patient outcomes.
Conclusion
This case report adds to the limited literature on renal cell carcinoma (RCC) metastasis to the small bowel and highlights the importance of recognizing this rare metastatic presentation. Small bowel metastasis should be considered in patients with a history of RCC who present with symptoms of acute intestinal obstruction. With the advent of targeted therapies patient survival has significantly improved. As a result, patients may live long enough to develop metastases at uncommon sites such as the small intestine. Therefore, metastatic RCC to the small bowel may be encountered more frequently than previously reported. Further cohort studies are required to better understand its true prevalence and clinical characteristics.
Contributors: HS: found the concept and participated in writing; HR: revised and approved the final manuscript; VL and BMB: participated in writing. HS will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study. Funding: None; Competing interests: None stated.
References - Padala SA, Barsouk A, Thandra KC, Saginala K, Mohammed A, Vakiti A, et al. Epidemiology of Renal Cell Carcinoma. World J Oncol. 2020;11(3):79-87.
- Starr A, Miller GM. Solitary jejunal metastasis twenty years after removal of a renal-cell carcinoma; report of a case. N Engl J Med. 1952;246(7):250-251.
- Vig SVL, Zan E, Kang SK. Imaging for metastatic renal cell carcinoma. Urol Clin North Am. 2020;47(3):281-291.
- Ismail I, Neuen BL, Mantha M. Solitary jejunal metastasis from renal cell carcinoma presenting as small bowel obstruction 19 years after nephrectomy. BMJ Case Rep. 2015;2015:bcr2015210857.
- Todorovic Ð, Stojanovic B, Filip M, Ðordevic Ð, Stankovic M, Jovanovic I, et al. Small bowel perforation due to renal carcinoma metastasis: A comprehensive case study and literature review. Diagnostics (Basel). 2024;14(7):761.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Sarma H, Ramesh H, Lekha V, Babu BMMetastatic Renal Cell Carcinoma to Small Bowel.JCR 2026;16:22-26 |
|
Sarma H, Ramesh H, Lekha V, Babu BMMetastatic Renal Cell Carcinoma to Small Bowel.JCR [serial online] 2026[cited 2026 May 18];16:22-26. Available from: http://www.casereports.in/articles/16/1/Metastatic-Renal-Cell-Carcinoma-to-Small-Bowel.html |

|
|
|
|
|