|
|
|
|
|
Obstructive Pyelonephritis Secondary to Ovarian Hyperstimulation Syndrome During IVF Treatment
|
|
|
|
Sara Haddad1, Youmna Saade2, Christiane Saade3 1Department of Medicine, Division of Infectious Diseases, Vanderbilt University Medical Center, Nashville, Tennessee, USA; 2School of Medicine, American University of Beirut, Beirut, Lebanon; 3Department of Obstetrics and Gynecology, Holy Spirit University of Kaslik, Kesrewan, Lebanon. |
|
|
|
|
|
Corresponding Author:
|
|
Dr Sara Haddad Email: Haddadsarah91@gmail.com |
|
|
|
|
|
|
|
|
Received:
03-NOV-2025 |
Accepted:
31-OCT-2025 |
Published Online:
05-APR-2026 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: Ovarian hyperstimulation syndrome (OHSS) is a known complication of controlled ovarian stimulation during in vitro fertilization (IVF). In severe cases, marked ovarian enlargement may lead to compression of adjacent structures. Urinary tract obstruction and subsequent pyelonephritis are rare but serious complications. Case Report: We report a woman undergoing IVF who developed severe OHSS and presented with fever, abdominal distension, and flank pain. Imaging revealed enlarged ovaries causing ureteric compression with resulting hydronephrosis and obstructive pyelonephritis. The patient was treated with intravenous antibiotics and supportive management, leading to clinical improvement. Conclusion: Obstructive pyelonephritis secondary to OHSS is an uncommon complication. Early recognition and prompt management are essential to prevent serious renal and systemic complications. |
|
|
|
|
|
Keywords :
|
Assisted Reproductive Techniques, Female Urogenital Diseases, Hydronephrosis, In Vitro Fertilization, Ovarian Hyperstimulation Syndrome, Pyelonephritis.
|
|
|
|
|
|
|
|
|
|
|
|
Introduction
Oocyte retrieval is one of the essential steps of an in vitro fertilization (IVF) cycle and since 1985 is performed via a transvaginal ultrasound guided approach [ 1]. Although this technique is preferred over laparoscopic or abdominal retrieval [ 2], it remains associated with possible occasional complications. Examples of these reported occasional difficulties may include hemorrhage, injury to adjacent organs, vaginal bleeding and occasionally reported pelvic abscesses and infections [ 3]. Some possible complications remain underreported specially in patients with underlying polycystic ovary syndrome (PCOS) who have a higher risk of ovarian hyperstimulation syndrome than the rest of the population undergoing IVF [ 4]. We report a case of obstructive pyelonephritis following oocyte retrieval in an IVF candidate with underlying PCOS.
Case Report
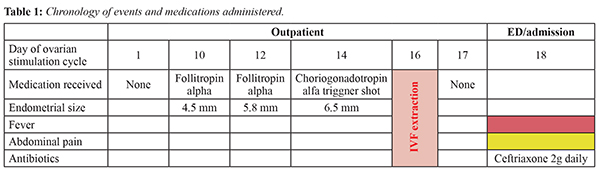
A 39-year-old woman, gravida 2 para 0 aborta 2, with a known history of polycystic ovary syndrome (PCOS) and no prior surgical history presented to the emergency department with severe abdominal pain that began two days after oocyte retrieval performed as part of an in vitro fertilization (IVF) cycle. Prior to the procedure, she had received a 14-day course of low-dose follitropin alfa injections, which resulted in an adequate ovarian response [Table 1]. Ovulation was triggered with a choriogonadotropin alfa injection, and follicular aspiration was performed 36 hours later. Two days after the procedure, she developed severe right-sided lumbar pain radiating to the right thigh, accompanied by a one-day history of intermittent nausea and vomiting. She denied any urinary symptoms. On presentation, she was febrile with a temperature of 38.7°C, blood pressure of 130/60 mmHg, and a heart rate of 92 beats per minute. The patient appeared fatigued but remained alert and oriented. Cardiovascular and respiratory examinations were unremarkable. Abdominal examination revealed marked right-sided costovertebral angle tenderness, while the abdomen was otherwise soft.
Initial laboratory investigations demonstrated leukocytosis with a white blood cell count of 17 K/µL and neutrophilic predominance, C-reactive protein of 168 mg/L, and hemoglobin of 13.7 g/dL [Table 2]. Urinalysis showed 60 white blood cells and more than 100 red blood cells per high-power field, with negative nitrite and leukocyte esterase tests. Urine culture obtained at admission later showed no bacterial growth. Contrast-enhanced abdominal computed tomography revealed right-sided hydroureteronephrosis suggestive of obstructive pyelonephritis [Fig.1] in the setting of multiple bilateral ovarian cystic enlargements consistent with ovarian hyperstimulation syndrome. Pelvic ultrasonography demonstrated an enlarged right ovary measuring approximately 7.5 cm. The patient was started on intravenous ceftriaxone 2 g daily. Following imaging findings, the urology team was consulted and the patient underwent cystoscopy with placement of a right-sided double-J ureteral stent. Purulent drainage was noted intraoperatively at the level of obstruction [Fig.2]. The collected purulent sample was sent for microbiological culture; however, results remained negative. The patient continued intravenous ceftriaxone during hospitalization and was subsequently transitioned to oral cefixime 400 mg daily to complete a total of 14 days of antimicrobial therapy. Her clinical condition improved following decompression and antibiotic treatment.
Discussion
Oocyte retrieval is generally considered a safe and well-tolerated procedure [ 3]. In 1985, transvaginal ultrasound-guided oocyte retrieval (TVOR) was first introduced for use in in vitro fertilization (IVF). Since then, it has become the gold standard technique for follicular aspiration due to its relative simplicity, minimally invasive nature, and high efficacy in assisted reproductive procedures [ 5]. Despite its favorable safety profile, complications related to transvaginal follicle aspiration have been reported, although their incidence remains low. Documented complications include vaginal perforation [ 6], hemorrhage, hemoperitoneum secondary to ovarian bleeding, injury to iliac vessels with subsequent pseudoaneurysm formation [ 7], trauma to adjacent pelvic organs, minor pelvic infections, and pelvic abscess formation [ 1, 7- 9]. Additional rare complications described in the literature include adnexal torsion, rupture of endometriotic cysts, anesthetic or neurological complications [ 10], and even vertebral osteomyelitis [ 11]. Although uncommon, urinary tract complications may occur, particularly in the presence of significantly enlarged ovaries. Excessive ovarian response during ovarian stimulation can result in increased ovarian size and hypervascularization, which may lead to compression of adjacent pelvic structures. Enlargement of the ovaries can exert pressure on surrounding organs, including the urinary tract. Compression of the bladder may manifest as pelvic pain, urinary frequency, and difficulty in bladder emptying. In more severe cases, pressure on the urethra may lead to urinary retention, a rare but potentially serious complication that interferes with normal urinary outflow and may result in bladder distension. Acute renal failure during ovarian stimulation has also been reported and is thought to result from ureteric compression [12]. Although ureteral injury following transvaginal ultrasound-guided oocyte retrieval is rare, it may result in serious complications such as fistula formation, ureteral obstruction, and renal dysfunction [14-17]. Infectious complications following oocyte retrieval procedures are rarely reported, although the procedure itself is not entirely without risk [3,18]. Known risk factors for infection following transvaginal oocyte retrieval include endometriosis, prior pelvic inflammatory disease (PID), previous pelvic surgery, and pelvic adhesions [18]. In addition, ovarian stimulation may predispose patients to urinary stasis and pelvic inflammation, which can increase the risk of urinary tract infections. Increased pressure on the bladder and altered micturition dynamics may contribute to recurrent urinary tract infections. Furthermore, certain assisted reproductive techniques involving urinary catheterization may further increase infection risk. Within this context of pelvic inflammation and mechanical compression, acute pyelonephritis may represent a serious complication associated with ovarian stimulation and enlarged ovarian size following oocyte retrieval. In this report, we describe a patient with polycystic ovary syndrome (PCOS) who developed ovarian hyperstimulation syndrome (OHSS) following an IVF procedure, which was subsequently complicated by obstructive pyelonephritis. This case suggests that patients with PCOS who develop hyperstimulation syndrome may be at increased risk of genitourinary infections, particularly upper urinary tract infections, due to possible mechanical obstruction of the urinary system caused by enlarged ovaries. To the best of our knowledge, this appears to be among the first reported cases in the literature where features suggestive of mild OHSS [4,19] may have contributed to the development of obstructive pyelonephritis. Management of such complications requires a multidisciplinary approach involving close clinical monitoring, symptomatic management, and, when necessary, targeted interventions such as antimicrobial therapy, hospitalization, or urological procedures. Early recognition and prompt treatment are crucial to achieving favorable outcomes. Although pelvic infection following oocyte retrieval is uncommon, its low incidence raises questions regarding the routine use of prophylactic antibiotics. Moreover, despite variations in the technique of transvaginal oocyte retrieval, there remains scope for improvement through the development and implementation of standardized clinical guidelines [1]. Finally, patients undergoing oocyte retrieval should be adequately counseled regarding the potential risks associated with the procedure. Physicians should provide accurate information on the incidence of possible complications, and these risks should be clearly documented in the written informed consent obtained prior to the procedure.
Conclusion
This case highlights the importance of maintaining a high index of suspicion for urinary tract complications in patients presenting with flank pain and fever after IVF procedures. Early recognition, prompt imaging, and timely multidisciplinary management are essential to prevent serious renal complications and ensure favourable patient outcomes.
Contributors: SH: Conceptualization, writing (original draft), writing (review and editing); YS: conceptualization, writing (original draft); CS: conceptualization, writing (original draft), writing (review and editing), supervision. SH will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study. Funding: None; Competing interests: None stated.
References - Gode F, Akarsu S, Isik AZ. Complications of Oocyte Retrieval. In: Textbook of Assisted Reproduction. 2020; (pp. 757-761). Singapore: Springer Singapore.
- Grynberg M, Berwanger AL, Toledano M, Frydman R, Deffieux X, Fanchin R. Ureteral injury after transvaginal ultrasound-guided oocyte retrieval: a complication of in vitro fertilization-embryo transfer that may lurk undetected in women presenting with severe ovarian hyperstimulation syndrome. Fertility and Sterility. 2011;96(4):869-871.
- Özaltin S, Kumbasar S, Savan K. Evaluation of complications developing during and after transvaginal ultrasound guided oocyte retrieval. Ginekologia Polska. 2018;89(1):1-6.
- Sun B, Ma Y, Li L, Hu L, Wang F, Zhang Y, Dai S, Sun Y. Factors associated with ovarian hyperstimulation syndrome (OHSS) severity in women with polycystic ovary syndrome undergoing IVF/ICSI. Frontiers in Endocrinology. 2021;11:615957.
- El-Shawarby SA, Margara RA, Trew GH, Lavery SA. A review of complications following transvaginal oocyte retrieval for in-vitro fertilization. Human Fertility. 2004;7(2):127-133.
- Cho MM, McGovern PG, Colon JM. Vaginal perforation during transvaginal ultrasound-guided follicle aspiration in a woman undergoing multiple cycles of assisted reproduction. Fertility and Sterility. 2004;81(6):1695-1696.
- Aragona C, Mohamed MA, Espinola MS, Linari A, Pecorini F, Micara G, et al. Clinical complications after transvaginal oocyte retrieval in 7,098 IVF cycles. Fertility and Sterility. 2011;95(1):293-294.
- Dicker D, Ashkenazi J, Feldberg D, Levy T, Dekel A, Ben-Rafael Z. Severe abdominal complications after transvaginal ultrasonographically guided retrieval of oocytes for in vitro fertilization and embryo transfer. Fertility and Sterility. 1993;59(6):1313-1315.
- Azem F, Wolf Y, Botchan A, Amit A, Lessing JB, Kluger Y. Massive retroperitoneal bleeding: a complication of transvaginal ultrasonography–guided oocyte retrieval for in vitro fertilization embryo transfer. Fertility and Sterility. 2000;74(2):405-406.
- Van Eenige MM, Scheele F, Van Haaften M, Westrate W, Jansen CA. A case of a neurological complication after transvaginal oocyte retrieval. J Assisted Reproduction and Genetics. 1997;14(1):21-22.
- Almog B, Rimon E, Yovel I, Bar-Am A, Amit A, Azem F. Vertebral osteomyelitis: a rare complication of transvaginal ultrasound-guided oocyte retrieval. Fertility and Sterility. 2000;73(6):1250-1252.
- Heldal K, Lyngdal PT, Johansen TE, Kahn JA. Acute renal failure following IVF: case report. Human Reproduction. 2005;20(8):2250-2252.
- Choudhary RA, Bhise NM, Mehendale AV, Ganla KN. Ureteric injury during transvaginal oocyte retrieval (TVOR) and review of literature. Journal of Human Reproductive Sciences. 2017;10(1):61-64.
- Fiori O, Cornet D, Darai E, Antoine JM, Bazot M. Uro-retroperitoneum after ultrasound-guided transvaginal follicle puncture in an oocyte donor: a case report. Human Reproduction. 2006;21(11):2969-2971.
- von Eye Corleta H, Moretto M, D'Avila ÂM, Berger M. Immediate ureterovaginal fistula secondary to oocyte retrieval a case report. Fertility and sterility. 2008;90(5):2006-e1.
- Mongiu AK, Helfand BT, Kielb SJ. Ureterovaginal fistula formation after oocyte retrieval. Urology. 2009;73(2):444-e1.
- Coroleu B, Lopez Mourelle F, Hereter L, Veiga A, Calderon G, Martinez F, et al. Ureteral lesion secondary to vaginal ultrasound follicular puncture for oocyte recovery in in-vitro fertilization. Human reproduction (Oxford, England). 1997;12(5):948-950.
- Steyaert SR, Leroux-Roels GG, Dhont M. Infections in IVF: review and guidelines. Human Reproduction Update. 2000;6(5):432-441.
- Balakumar V, Ramalingam M, Kay V. Ovarian hyperstimulation syndrome. Obstetrics, Gynaecology & Reproductive Medicine. 2017;27(12):357-362.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Haddad S, Saade Y, Saade CObstructive Pyelonephritis Secondary to Ovarian Hyperstimulation Syndrome During IVF Treatment.JCR 2026;16:27-32 |
|
Haddad S, Saade Y, Saade CObstructive Pyelonephritis Secondary to Ovarian Hyperstimulation Syndrome During IVF Treatment.JCR [serial online] 2026[cited 2026 May 18];16:27-32. Available from: http://www.casereports.in/articles/16/1/Obstructive-Pyelonephritis-Secondary-to-Ovarian-Hyperstimulation-Syndrome-During-IVF-Treatment.html |

|
|
|
|
|