|
|
|
|
|
Unusual and Rare Presentation of Sternal Tuberculosis
|
|
|
AK Dawar, Richa Dawar, Kunal Gawri
From the Department of Orthopaedics,
ESI Hospital, Okhla, New Delhi. |
|
|
|
|
|
Corresponding Author:
|
Dr. A.K.Dawar
Email: dawar101@gmail.com |
|
|
|
|
|
|
|
|
Received:
07-OCT-2012 |
Accepted:
17-OCT-2012 |
Published Online:
30-OCT-2012 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Sternal tuberculosis is rare and not well documented, except for a few small series and case reports. Absence of external manifestations like swelling or sinus over the sternum makes its diagnosis difficult especially when patient presents with only chest pain. High index of suspicion helps in diagnosing the condition early so that antitubercular treatment can be started as soon as possible. Here, we report a rare case of manubrial tuberculosis who presented with undiagnosed chest pain for one year.
|
|
|
|
|
|
Keywords :
|
Sternal Tuberculosis, Manubrium, Chest pain
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff44e1010000000f01000001000100 6go6ckt5b5idvals|150 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext
Even today tuberculosis is an endemic disease in developing countries. Its incident is rising due to spread of HIV and development of multi- drug resistant tuberculosis. According to WHO report [1] of 2009, regions of South East Asia, Western Pacific and Africa accounted for 86% of global cases of tuberculosis in 2007. Despite reductions in the global burden of TB, 37% of smear-positive TB cases are not being treated, more than 90% of multidrug resistant TB (MDR-TB) are not being diagnosed and treated, the majority of HIV-positive tuberculosis patients do not know their HIV status, and those who do are not yet accessing antiretroviral therapy [1]. Skeletal TB accounts for 1-3% of all patients with tuberculosis. Approximately 60-80% of skeletal tuberculosis cases involve spine or weight bearing joints while sternum is involved in 1% of cases [2-4]. Primary tuberculous sternal osteomyelitis is even more uncommon. Often the diagnosis of sternal tuberculosis is not made until the disease is well advanced with only 25 cases reported in peer reviewed journals in post anti- tuberculosis therapy (ATT) era [5].
Case Report
A 44 year old non-diabetic male presented with pain in upper central chest (manubrial area) for 9 months. along with tenderness over costochondral junctions on both sides of manubrium. The pain was not associated with swelling or any inflammation. There was no history of chest infection, fever or any other constitutional symptoms. General physical examination did not reveal any significant lymphadenopathy. His systemic examination was unremarkable. Accordingly, he was treated for costochondritis with NSAIDS without any improvement. Subsequently, he was investigated for heart disease and his chest X-ray, electrocardiogram, echocardiography and treadmill test were negative. Non response to pain killers prompted a search for underlying disorder. Laboratory results showed TLC 9000 with differential of P61 L36 ESR 28mm. HIV and C-reactive protein were negative. Mantoux was reported to be 20 mm. Later, his chest pain progressed to involve right side over the lower ribs along with fever. Sputum examination was negative for acid fast bacilli. CECT chest suggested a diagnosis of sternal tuberculosis revealing destructive lesion of manubrium with some enlarged mediastinal lymph nodes [Fig.1]. Repeat X-ray of the chest showed right sided pleural effusion [Fig.2]. Aspirate from effusion was negative for acid fast bacilli but PCR was positive for tuberculosis. CT guided needle biopsy from sternum yielded haemorrhagic fluid which was negative for AFB. Open curettage biopsy of the manubrium was done. Histopathology examination revealed classical picture of tuberculosis with caseous necrosis and epitheloid giant cells. He was put on directly observed treatment, short course anti-tuberculous therapy and his chest pain gradually subsided.
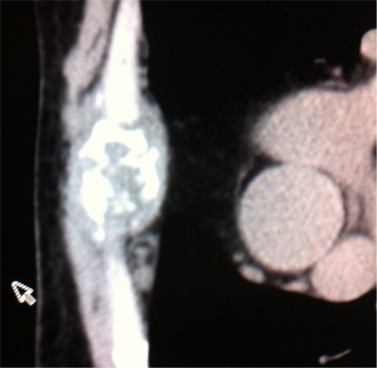 Fig.1 : CT scan of sternum showing destructive lesion
Fig.1 : CT scan of sternum showing destructive lesion
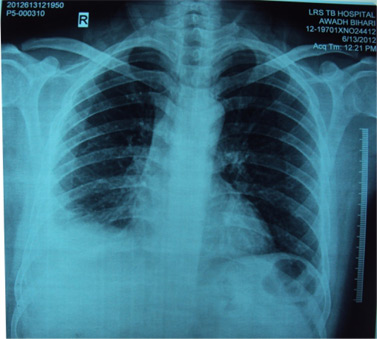 Fig.2 : Chest X ray with right sided pleural effusion
Fig.2 : Chest X ray with right sided pleural effusion
Discussion
Thoracic skeletal tuberculosis commonly involves costo-verteberal or costochondral junctions. Sternum was involved in 0-7% of all cases of thoracic TB cases in a series from England, South Arabia and India [6-7]. In 81% cases, sternal TB presents with a soft tissue swelling over sternum, painful bony swelling, erythema, warmth, tenderness, enlarged lymph nodes, bony deformity or fracture, draining abscess or sinuses and constitutional symptoms are less commonly seen [8]. As per literature, clinical manifestations of tuberculosis are present for 2 months to 6 years before diagnosis of sternal tuberculosis is made [8]. 40% cases of sternal TB have evidence of tuberculosis on other sites than sternum with lymphatic system being the most common. Lesions of sternal body are more common than of manubrium. Lesion of manubrium can be complicated by spread to sternocostal joints. As stated earlier almost all cases of sternal TB reported in literature had visible lesion (swelling, erythema, chronic sinuses etc.) before they were diagnosed as sternal TB. Miten Vasa [8] has reported a case where patient was treated for painful muscles of neck, shoulder and costochondritis for many months before being diagnosed as sternal tuberculosis. However, he was diagnosed as sternal tuberculosis only after he developed erythmatous swelling of manubrium. Probably our case is the only case who was diagnosed as sternal TB as cause of anterior chest pain without any external evidence of tuberculosis. Since persistent bone pain, nonresponsive to analgesics is characteristic of tuberculosis or neoplasm, CT or MRI should be done when X-ray is normal in such cases [9].
Treatment of sternal TB is controversial. Many authors recommend surgical debridement to prevent recurrence or formation of draining sinuses [10-12]; however, there are no formally defined surgical indications in the literature.
Conclusion: Tuberculosis occurring in an unusual location like manubrium, may complicate the differential diagnosis. We would like to emphasize that clinicians should have a high index of suspicion for tuberculosis when a patient with chest pain nonresponsive to analgesics, presents with positive mantoux test.
References
- World Health Organization. Global tuberculosis control – epidemiology, strategy, financing: WHO Report 2009.<http://www.who.int/tb/publications/global_report/2009/en/index.html>. Accessed on 28 September 2012.
- Zhao X, Chen S, Deanda AJ, Kiev J. A rare presentation of tuberculosis. Am Surg 2006;72: 96-97.
- Martini M, Cuahes M. Bone and joint tuberculosis: A review of 652 cases. Orthopedics 1988;11:861-866.
- Davies PD, Humphries MJ, Byfield SP, Nunn AJ , Darbyshire JH , Citron KM , et al. Bone and joint tuberculosis: A survey of notifications in England and Wales. J Bone Joint Surg Br 1984;66:326-330.
- Bajracharya, S, Singh GK, Singh M. Primary tubercular osteomyelitis of the sternum: Report of two cases. Internet J Third World Med 2007; 5(2). <www.ispub.com/journal/the_internet_journal_of_third_world_medicine.html>. Accessed on 28 September 2012.
- Dhillon MS, Gupta RK, Bahadur R, Nagi ON. Tuberculosis of the sternoclavicular joints. Acta Orthopaedica 2001;72:514-517.
- McLellan DG, Philips KB, Corbett CE, Bronze MS. Sternal osteomyelitis caused by mycobacterium tuberculosis: Case report and review of the literature. Am J Med Sci 2000;319:250-254.
- Vasa M, Ohikhuare C, Brickner L. Primary sternal tuberculosis osteomyelitis: A case report and discussion. Can J Infect Dis Med Microbiol 2009;20(4):181-184.
- Vohra R, Kang HS, Dogra S, Saggar RR, Sharma R. Tuberculous osteomyelitis. J Bone Joint Surg Br 1997;79:562-566.
- Ford SJ, Rathinam S, King JE, Vaughan R. Tuberculous osteomyelitis of the sternum: Successful management with debridement and vacuum assisted closure. Eur J Cardiothorac Surg 2005;28:645-647.
- Hsu HS, Wang LS, Wu YC, Fuhn HJ, Huang MH. Management of chest wall tuberculosis. Scand J Thorac Cardiovasc Surg 1995;29:119-123.
- O’Brien DP, Athan E, Hughes A, Johnson PD. Successful treatment of Mycobacterium ulcerans osteomyelitis with minor surgical debridement and prolonged rifampicin and ciprofloxacin therapy: A case report. J Med Case Rep 2008;2:123.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Dawar AK, Dawar R, Gawri KUnusual and Rare Presentation of Sternal Tuberculosis.JCR 2012;2:83-85 |
|
Dawar AK, Dawar R, Gawri KUnusual and Rare Presentation of Sternal Tuberculosis.JCR [serial online] 2012[cited 2026 May 21];2:83-85. Available from: http://www.casereports.in/articles/2/2/unusual-and-rare-presentation.html |

|
|
|
|
|