6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1fffc17020000001901000001000700
6go6ckt5b5idvals|166
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Jejunal diverticula are rare with an incidence of less than 1.5% [1]. Pathologically, they are pseudodiverticula of the pulsion type, resulting from increased intra-luminal pressure and weakening of the bowel wall. Most cases of jejunal diverticulosis remain asymptomatic. Few complications such as chronic abdominal pain, malabsorption, haemorrhage, diverticulitis, obstruction, abscess formation and rarely diverticular perforation have been reported in 10 to 30% of patients [2-4].
Case Report
A 65 year old male presented with off and on pain in the upper abdomen since last 2 and half years. There was a history of dyspepsia, belching, discomfort and vomiting after meals. Since last 7 days the pain increased in severity along with absolute constipation and visible bowel loops in the upper abdomen. He developed high grade fever with chills and coffee brown copious vomiting since last 2 days.
On examination he had a toxic look. He was dehydrated, febrile and anaemic with a coated tongue. He had a temperature of 101°F, pulse 105/min, blood pressure 90/50 mm Hg, respiratory rate 16 breaths/min and an oxygen saturation of 95%. Abdominal examination revealed a generalized tenderness and signs of peritonitis with absence of bowel sounds. Per-abdominal examination showed rigidity and rebound tenderness with visible bowel loops. Ryle’s tube aspiration was haemorrhagic.
Laboratory investigations revealed Hb 8.6 g/dl, TLC 18200 cells/mm3, DLC P80L20, Urea 18.6 mg/dl and Creatinine 1.1mg/dl. General blood picture showed presence of toxic granulations and features of macrocytic anemia. Serum protein levels were markedly reduced. Abdominal X-ray displayed multiple dilated loops of small bowel. CT scan of the abdomen and pelvis revealed thickening of the duodenum and dilatation of the proximal jejunum. Multiple small bowel diverticula were identified with surrounding pockets of free air adjacent to the jejunal diverticula suggestive of perforation.
A midline exploratory laparotomy revealed several variable sized diverticula present from duodeno-jejunal junction to 35 cm of jejunum; four of which were situated at the mesenteric border and two at the anti-mesenteric border. The entire segment of jejunum containing multiple diverticula was inflamed, edematous and adhered badly with each other and the surrounding adnexa with the development of gangrene. After mobilization, the jejunal loop containing the diverticula was excised and end-to-end anastomosis was carried out in a single layer using vicryl 2-0. The abdomen was irrigated and a drain was left near the anastomosis site.
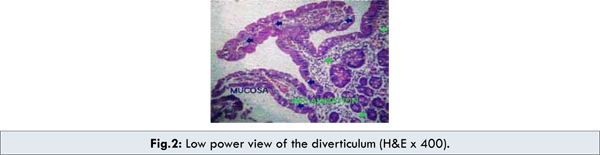
Grossly, there was a 5-cm segment of small bowel with multiple diverticula [Fig.1]. The diverticular wall consisted only of mucosa. There was no muscularis propria in the wall of the diverticulum. There was inflammatory cell infiltration in the layers [Fig.2] with no evidence of malignancy. Post-operative period was uneventful with improvement in his hemoglobin levels and correction in the macrocytic picture within 2 months of surgery.
Discussion
Jejunal diverticula are the least common type of small bowel diverticula [1]. The actual incidence of both types of diverticula is not known because these lesions are usually asymptomatic. Autopsy studies reveal an incidence between 1.3% and 4.6%, whereas radiologic studies show an incidence between 0.02% and 2.3% [1,5]. Jejunal diverticula make up only 8% of all small bowel diverticula and are associated with diverticula of other areas, with colonic involvement observed in up to 50% of cases [6]. Duodenal diverticula are 5 times more common than jejuno-ileal. Duodenal diverticula occur in equal numbers of men and women, while a slight male preponderance is noted in jejuno-ileal diverticula. Most cases of duodenal diverticula are observed in patients older than 50 years, while jejuno-ileal diverticula are commonly observed in patients aged 60-70 years [1].
Although the true aetiology of jejunal diverticulosis is unknown, it is believed to develop from a combination of abnormal peristalsis, intestinal dyskinesis, and high segmental intra-luminal pressure. These pulsion-type false diverticula occur along the mesenteric border of the intestine, where blood vessels pierce the muscularis layer of the bowel wall, causing weak areas to develop. These weak areas lead to herniation of mucosa, submucosa, and serosa while excluding the muscularis layer.
Usually, this disorder is asymptomatic until it presents with associated complications. Complications warranting surgical intervention occur in 8 to 30% of patients and include pain, bleeding, diverticulitis, intestinal obstruction, constipation, nausea, vomiting, perforation and localized abscess with or without signs of peritonitis, malabsorption, anemia, biliary colic, volvulus orenteroliths [6]. Jejunal diverticulitis occurs with a frequency of 2.3% in patients with known diverticulosis [4]. The aetiology is thought to be secondary to luminal obstruction leading to bacterial stasis and a localized inflammatory reaction. Diverticulitis may be further complicated by perforation with peritonitis, mechanical obstruction or fistulisation.
Jejunal diverticulosis often presents a diagnostic dilemma. Abdominal radiographs and/or chest radiographs may demonstrate evidence of perforation, such as free air under the diaphragm or peritoneum; evidence of intestinal obstruction, or evidence of ileus, including multiple air-fluid levels and bowel dilatation. CT scan may identify thickening, inflammation or localized abscess formation [2,3]. Endoscopic procedures, such as double-balloon enteroscopy and capsule endoscopy, are useful in diagnosing small-bowel disorders [7]. However, these procedures cannot be used during emergency. Diagnostic laparoscopy can be very useful in investigating patients with a complicated symptomatology avoiding the need for unnecessary laparotomy. Enteroclysis is thought to be the best diagnostic tool for visualizing this disease because the positive pressure that results from instillation of barium and insufflation causes the diverticula in the bowel lumen to become prominent. Laboratory studies tend to be nonspecific, but an elevated WBC count with shift to left favours diverticulitis or perforation.
Management of jejunal diverticula depends on the presenting symptoms. It is recommended that asymptomatic diverticula found incidentally during laparotomy for other reasons should be left alone [7,8]. Surgery is required in approximately 8.5% of all patients with jejunal diverticula, although it increases to 40% in patients with symptoms or complications [9]. Localization of the diverticula may be difficult during laparotomy because they are frequently hidden between the mesenteric leaves. Resection of the surrounding small bowel with primary anastomosis is recommended for complicated diverticula. Extensive resection of multiple diverticula may lead to short bowel syndrome. Simple diverticulectomy is not recommended because it has been linked to postoperative leakage, sepsis, and death.
The mortality rate of complicated jejunal disease reported earlier ranged between 21% and 30% [8]; however, some recent reviews indicate a reduced rate between 0% and 5% probably due to improvement in the intensive care management and antimicrobial treatment [4].
Conclusion
Jejunal diverticula are rare and usually asymptomatic. However, they may lead to chronic non-specific abdominal symptoms or rarely, as displayed by this case, can present as acute abdomen. Jejunal diverticulosis in the elderly can lead to significant morbidity and mortality and so should be suspected in those presenting with crampy abdominal pain and altered bowel habits. Once diagnosed, conservative medical management should be instituted to alleviate symptoms and reduce the risk of complications. Rarely, jejunal diverticular disease may present as intestinal perforation, for which surgical repair is the treatment of choice.
References
Matteoni R, Lolli E, Barbieri A, D’Ambrosi M. Perforated jejunal diverticulitis: personal experience and diagnostic with therapeutical considerations. Ann Ital Chir. 2000;71:95-98. PMID:10829530- Zager JS, Garbus JE, Shaw JP, Cohen MG, Garber SM. Jejunal diverticulosis: a rare entity with multiple presentations, a series of cases. Dig Surg. 2000;17:643-645. PMID:11155015
- Woods K, Williams E, Melvin W, Sharp K. Acquired jejunoileal diverticulosis and its complications: a review of the literature. Am Surg. 2008;74:849-854. PMID: 18807676
- Akhrass R, Yaffe MB, Fischer C, Ponsky J, Shuck JM. Small-bowel diverticulosis: perceptions and reality. J Am Coll Surg. 1997;184:383-388. PMID:9100684
- RossCB, Richards WO, Sharp KW, Bertram PD, Schaper PW. Diverticular disease of the jejunum and its complications. Am Surg. 1990;56: 319-324. PMID: 2110429
- Lee RE, Finby N. Jejunal and ileal diverticulosis. AMA Arch Intern Med. 1958;102:97-102.
- Sibille A, Willocx R. Jejunal diverticulitis. Am J Gastroenterol. 1992;87:655-658. PMID: 1595658
- Chendrasekhar A, Timberlake GA. Perforated jejunal diverticula: an analysis of reported cases. Am Surg. 1995;61:984-988. PMID: 7486432
- Rodriguez HE,Ziauddin MF, Quiros ED, Brown AM, Podbielski FJ.Jejunal diverticulosis and gastrointestinal bleeding. J Clin Gastroenterol. 2001;33:412-414.