|
|
|
|
|
Ischemic Stroke in Young due to Combined Protein C and S Deficiency
|
|
|
ML Patel, Rekha Sachan1, KK Gupta, Ganesh Seth
From the Department of Medicine and Obstetrics & Gynaecology1,
King George’s Medical University, Lucknow-226003, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. ML Patel
Email: apatelsac@gmail.com |
|
|
|
|
|
|
|
|
Received:
14-NOV-2012 |
Accepted:
27-DEC-2012 |
Published Online:
15-JAN-2013 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
WHO defines stroke as an event caused by the interruption of the blood supply to the brain, usually because a blood vessel bursts or is blocked by a clot. This cuts off the supply of oxygen and nutrients, causing damage to the brain tissue [1]. Globally, stroke is the third commonest cause of mortality [2] and the fourth leading cause of disease burden [3]. Ischemic stroke is the most common cerebrovascular disease, most often due to atherothrombotic diseases and uncommonly by disorders of hypercoagulation. Disorders of coagulation leading to thrombotic disorders are approximately 1% of all ischemic strokes and 4-8% of young strokes. Similarly combined deficiency of protein C and S can lead to hypercoagulable state and rarely present as cerebrovascular accident. We describe here a rare case of 27 year old male who presented with right middle cerebral artery territory infarct due to combined protein C and S deficiency. |
|
|
|
|
|
Keywords :
|
Stroke, Blood Coagulation, Protein C, Infarction, Middle Cerebral Artery, Brain.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffc41f020000001901000001000d00 6go6ckt5b5idvals|167 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Cerebrovascular diseases are one of the common causes of high morbidity and mortality all over the world and out of all cerebrovascular diseases most of them are ischemic strokes (85%). Stroke in young individual poses a major problem as these young family members are the major income earner of the family. Abraham et al [4] from Vellore, South India reported that 25% cases of the stroke were less than 40 years of age. Other Indian studies have highlighted a high incidence 24-35% of stroke in young population [5]. Atherothrombotic diseases are most common cause for ischemic stroke, however disorder of coagulation although uncommon but can lead to hypercoagulability resulting in ischemic stroke.
Case Report
A 27 year old male presented with complains of weakness in left side of body since last 10 days. General physical examination was unremarkable. Neurological examination revealed findings consistent with left-sided hemiparesis. No precipitating factors such as obesity, diabetes, hypertension, valvular heart disease, chronic drug intake, intravenous drug abuse and smoking were present. Family history was negative for vascular events or other predisposing factors for stroke. On examination motor power was decreased in the left side of body (III/V) along with right upper motor neuron facial palsy. Other systemic examination was within normal limit.
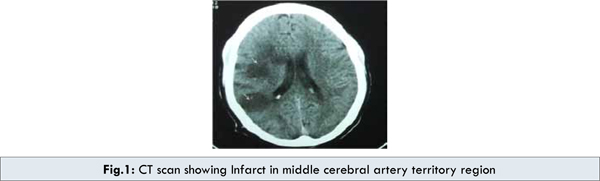
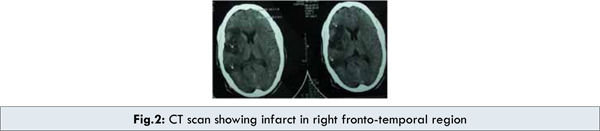
Routine investigation revealed hemoglobinof 13gm/dl, leucocyte count 12000/dL, platelet count 1.52 lac/mm3 with hematocrit of 39%, ESR 28 mm, prothrombin time 13 seconds (control 12 second), INR 1.1 and activated partial prothrombin time 22 seconds (control 20 seconds). Urine analysis, chest X-ray and fundus examination were unremarkable. Renal and liver function tests were within normal range. Ultrasonography abdomen and continuous wave Doppler sonography study in extracranial carotid, vertebral arteries and in all four limbs was normal. Transthoracic and transesophageal echocardiography did not reveal any abnormality. Laboratory findings including antinuclear factor, antiphospholipid antibodies and VDRL titer were normal. Factor V Leiden mutation was not detected. Protein C level was 38 units/ml (normal 67-195 units/ml), protein S level was 20 units/ml (normal 55-123 units/ml) and antithrombin III level was 88 units/ml (normal 70-122 units/ml) with normal serum homocystiene level and lipid profile. CT scan of head showed large infarct in right fronto-temporal region. CT angiography was done which showed large wedge shaped hypodense area suggesting infarct in right fronto-temporo-perietal region [Fig.1,2].
Differential diagnosis of ischemic stroke occurring secondary to antiphospholipid antibodies, hyperhomocy-steinemia, high plasma levels of fibrinogen, hypofibrinolysis, and resistance to activated protein C was kept. After initial therapy with heparin, the patient was kept on oral warfarin for long term anticoagulation.
Patient was discharged from hospital in good condition after two weeks with satisfactory outcome at 3 months follow up.
Discussion
Stroke means different pathological processes, all of them having as an end point the focal cerebral ischemia. 85% of the strokes are ischemic and 15% hemorrhagic. The importance of thrombophilic disorders in arterial stroke has been debatable. Even among the patients with ischemic stroke, a number of pathologically different processes are responsible as cardioembolism, large artery disease with arteriolosclerosis and thromboembolism, and small artery disease. Protein C is a vitamin K- dependent plasma protein that acts first as an anticoagulant by proteolytically degrading the activated factor V and inactivating factor VIII and secondly facilitates thrombolysis by its fibrinolytic activity. Protein S serves as a cofactor for protein C in its anticoagulant properties [6]. The relevance of deficiencies of these naturally occurring anticoagulants for venous thrombosis or pulmonary embolism is widely accepted.
The prevalence of protein C, S and antithrombin III in ischemic stroke varies up to 23% in different studies [7]. Protein C deficiency has occasionally been associated with arterial ischemic stroke [8]. In a meta-analysis published in 2003, reports of cases and studies regarding the deficiencies of proteins C, S, antithrombin, and factor V Leiden in ischemic strokes were mentioned. Protein C deficiency was found in only one of the 329 patients aged between 15 and 45 years. The conclusion of the meta-analysis was that it appears that protein C deficiency is weakly associated with the arterial stroke [9].
Protein S deficiency has been associated with cerebral arterial ischemia more often than protein C deficiency. Studies from Indian scenario and other countries shows conflicting reports limit the reliability of this association. Girolami et al. [10] and Sie et al. [11] were among the first who reported the association of familial deficiency of protein S as a cause of ischemic stroke in young. Mayer et al. [12] also supported the fact that acquired deficiency of free protein S is not a major risk factor for ischemic stroke. Douay et al. [13] reported that hereditary deficiencies of coagulation inhibitors are rare in ischemic stroke patients under 45 years and their systematic detection seems to be of poor interest. Wiesel et al. [14] studied 105 patients with protein S deficiency, out of which 14 had arterial thrombotic accidents involving the central nervous system or the myocardium, while most studies revealed a weaker association between these two [12].
A Swedish study of 107 patients aged between 18 and 44 years found only one with protein S deficiency, this meta-analysis describes case-reports and studies published until 2003 regarding this subject: they reported a frequency of this deficiency of 13.8% (5/36), 19% (8/35), 23% (19/98) in patients aged less than 45 years and 6% (4/66) in patients aged less than 60 years [9]. In this last study, all protein S deficiency patients had elevated anticardiolipin antibodies. This study suggests an association between antiphospholipid syndrome and protein S deficiency in ischemic stroke patients.
Antithrombin deficiency has only rarely been associated with stroke. Different studies show frequencies of 5% (3/66), 8% (5/60), but there were studies that reported just one case, thus, the evidence linking antithrombin deficiency with arterial stroke is weak [9].
The factor V Leiden mutation, the cause of activated protein C resistance (in 90% of cases) is the most common inherited coagulopathy associated with stroke. A study performed in Turkey and published in 2005, on 29 children with ischemic stroke and 20 with intracerebral hemorrhage, all of whom were compared with 20 controls. The authors found no evidence of an association between factor V Leiden mutation and ischemic stroke or intracerebral hemorrhage. The conclusion was that factor V Leiden mutation did not seem to be associated with a risk of cerebrovascular disease [15]. The risk of a stroke is high for person with factor V Leiden combined with other vascular risk factors, such as smoking and contraceptive use. A study investigated the prevalence of these mutations in 468 patients with an acute stroke or transient ischemic attack (TIA) before the age of 60 and in a healthy control population individually matched for age and gender. A significant interaction between the factor V Leiden, smoking, and risk of stroke in women was found: female smokers without the factor V Leiden had a somewhat increased risk of stroke of 2.6 (95% CI, 1.5 to 4.6; P=0.001) compared with nonsmoking non-carriers of the factor V Leiden. No such interaction was observed in men [16].
Conclusion
It is thus emphasised that Protein C deficiency though rarely associated with thrombotic events but when dealing with a case of cerebral infarction (arterial thrombosis) in young patient, screening for Protein C and S should be made, especially when patients are below 45 years, have a personal history of recurrent thrombosis without precipitating factors, thrombosis in unusual sites, thrombosis during pregnancy, a positive family history of thrombosis. A positive result requires immediate initiation of anticoagulant therapy.
References
- WHO. Stroke, Cerebrovascular accident. August 2010, http://www.who.int/topics/cerebrovascular_accident/en/. Accessed on 14 Nov 2012.
- Warlow C, Sudlow C, Dennis M, Wardlaw J, Sandercock P. Stroke. Lancet. 2003;362:1211–1224.
- Strong K, Mathers C, Bonita R. Preventing stroke: saving lives around the world. Lancet Neurology. 2007;6:182–187.
- Abraham J, Rao PS, Inbaraj SG, Shetty G, Jose CJ. An epidemiological study of hemiplegia due to stroke in South India. Stroke 1970;1:477-481.
- Bansal BC, Prakash C, Jain AL, Brajimanandan KRV. Cerebrovascular disease in young individuals below the age of 40 years. Neurol India. 1973;21:1-18.
- Clouse LH, Comp PC. The regulation of hemostasis: The protein C system. N Engl J Med. 1986;314:1298-1304.
- Bushnell CD, Goldstein LB. Diagnostic testing for coagulopathies in patients with ischemic stroke. Stroke. 2000;31:3067–3078.
- Hirsh J, Colman RW, Marder VJ, Clowes A, George JN. Overview of thrombosis and its treatment. In: Colman RW, Hirsh J, Marder VJ, Clowes A, George JN (editors): Hemostasis and Thrombosis. Basic Principles and Clinical Practice. 4th edition. Philadelphia: Lippincott Williams and Wilkins; 2001, pp. 1071–1084.
- Moster M. Coagulopathies and arterial stroke. Journal of Neuro–Ophthalmology. 2003;23(1):63–71.
- Girolami A, Simioni P, Lazzaro AR, Cordiano I. Severe arterial thrombosis in a patient with protein S cerebral deficiency (moderately reduced total and markedly reduced free proteinS): A family study. Thromb Haemost. 1989;61:144-147.
- Sie P, Boneu B, Bierme R, Wiesel ML, Grunebaum L, Cazenave JP. Arterial thrombosis and protein S deficiency. ThrombHaemost 1989;62:1040.
- Mayer SA, Sacco RL, Hurlet-Jensen A, Shi T, Mohr JP. Free protein S deficiency in acute ischemic stroke. A case-control study. Stroke. 1993;24:224-227.
- Dovay X, Lucas C, Caron C Goudemand J, Leys D. Antithrombin, protein C and protein S in 127 consecutive young adults with ischemic stroke. Acta Neurol Scand. 1998;98:124-127.
- Wiesel ML, Borg JY, Grunebaum L, Vasse M, Levesque H, Bierme R, Sie P. Influence of protein S deficiency on the arterial thrombosis risk. Presse Med. 1991;20:1023-1027.
- Buyru N, Altinisik J, Somay G. Factor V Leiden Mutation in Cerebrovascular Disease. Clinical and Applied Thrombosis/Hemostasis. 2005;11:339–342.
- Lalouschek W, Schillinger M. Matched Case–Control Study on Factor V Leiden and the Prothrombin G20210A Mutation in Patients With Ischemic Stroke/Transient Ischemic Attack Up to the Age of 60 Years. Stroke. 2005;36:1405–1410.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Patel ML, Sachan R, Gupta KK, Seth GIschemic Stroke in Young due to Combined Protein C and S Deficiency.JCR 2013;3:19-23 |
|
Patel ML, Sachan R, Gupta KK, Seth GIschemic Stroke in Young due to Combined Protein C and S Deficiency.JCR [serial online] 2013[cited 2026 Jun 6];3:19-23. Available from: https://www.casereports.in/articles/3/1/ischemic-stroke-in-young.html |

|
|
|
|
|