6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff54fc030000001e02000001000300
6go6ckt5b5idvals|242
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Despite the fact that the blue print of the whole body is unravelled, faultlessly during the growth and development of an animal; but amazingly variations do occur. The venous drainage of head and neck is provided with a paired triple jugular system comprising of superficial (Anterior and External jugular vein) and deep (Internal jugular vein) vessels. IJV collects the blood from the interior of the cranium whereas the EJV collects the same from the exterior of the cranium and deep part of the face [
1]. Both veins are being used in this era of critical care medicine for various life supporting interventions like central venous pressure monitoring, pulmonary artery catheter insertion & wedge pressure monitoring, emergency dialysis, transvenous cardiac pacing, administration of essential lifesaving drugs and total parenteral nutrition [
2]. Isolated variations of either formation and/ tributaries involving either external and/ internal jugular veins were recorded on either of the two side of the face but the combination of all such variations forms a rarest case. Unilateral IJV variations were found in 17.3% and bilateral variations were discovered in 8.7% patients [
3]. However, no reports mentioned the incidence of EJV variations except innumerable case reports. Significant variation in the anatomic location and size of jugular veins and unreliability of the external landmarks may be the cause for failure and complications of venous cannulation. This case may be useful for surgeons, radiologists and interventional anesthetists as this variation has not been previously mentioned in the literature.
Case Report
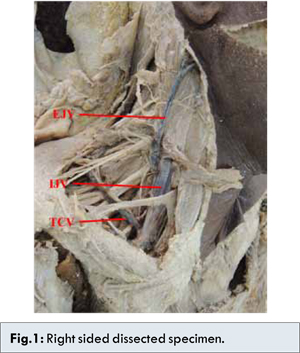
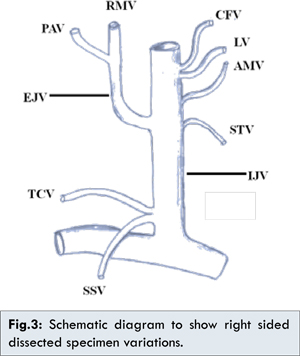
During routine dissection, we noted an anomalous venous formation and drainage on both the sides of a 45 year male cadaver. The veins of the neck were carefully dissected and the surrounding structures were delineated. Following variations were noted: On the right side of the neck, the External jugular vein (EJV) was formed by the union of an undivided retromandibular vein emanating from the parotid and the posterior auricular vein near the angle of the mandible. Formed EJV crosses the sternomastoid superficially and joins with IJV in the carotid triangle. IJV in its usual course receives the tributaries from the facial vein, lingual vein, and also from the anterior median vein of the neck, which is supposed to be drain into EJV. Further, below the carotid triangle IJV receives the superior thyroid as a normal tributary and in addition, transverse cervical and suprascapular veins as tributaries before it opened into the right subclavian vein [Fig.1].
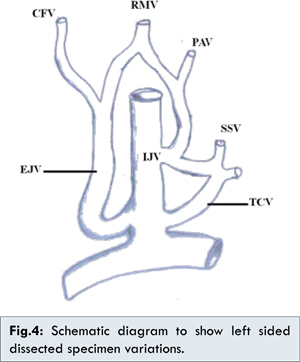
Dissection of the left side of the neck also shows complex venous malformation. The retromandibular vein divides into anterior and posterior branches below the apex of the parotid gland. As usual its anterior branch unites with the common facial vein to form EJV which in turn unites with IJV. The posterior branch of retromandibular and posterior auricular veins unites to form an unnamed vein and opened into IJV and also communicates with a common channel formed by the transverse cervical, suprascapular and some unnamed veins. Later the common channel drain into left subclavian vein [Fig.2].
Discussion
Generally, EJV is formed by the union of the posterior auricular and posterior division of the retromandibular vein which then receives the transverse cervical, suprascapular veins, and a communicating branch from the jugular venous arch before it open into the same side subclavian vein. In contrast, IJV begins as superior jugular bulb at the base of the skull receives the facial, lingual, thyroid, and pharyngeal veins drain into the same side brachiocephalic vein [
1].
In contrast to the above-mentioned literature, in the present report, the external jugular vein formed by the undivided retromandibular and posterior auricular vein on the right side of the face and by the union of anterior division of the retromandibular and facial vein on the left side of the face. On both side, they passed at first superficial to the sternocleidomastoid and then obliquely downwards and medial to it to drain into the internal jugular vein on both the sides of the face [Fig.3,4]. Yadav et al, reported a similar case but unilateral where the external jugular vein crossed superficially to the sternocleidomastoid muscle and ended in the internal jugular vein, above the level of the superior belly of omohyoid muscle [
4]. Hollished is of the opinion that in 1/3rd of his cases, EJV ended in IJV of the same side [
5]. Deslaugiers and his co-workers found that EJV drained into the trunk of IJV in 4% cases, Kopuz and Akan reported similar findings in only 2% of cases [
6,
7].
Normally, EJV receives the transverse cervical and suprascapular veins but in present case the said veins drain into the IJV on both side but with slight changes in the mode of their termination. This finding is consistent with the earlier report by Hollished [
5]. On the left side, an unnamed vein formed by the posterior division of the retromandibular and posterior auricular vein passes behind the sternocleidomastoid and drain in the IJV and also, communicates with the trunk formed by the larger left transverse cervical, left suprascapular and an unnamed vein from the upper limb. Available literature search yielded no such malformation.
Hollinshead also described variable communications of the anterior jugular vein with the internal jugular or facial vein [
5]. Present observations report the larger anterior jugular vein draining and terminating into internal jugular after joining the common facial vein and lingual vein. On the left side, anterior jugular vein drained into EJV. The location of IJV in relation to carotid artery was recorded as anterolateral, lateral and anterior. Anterolateral and lateral were considered as safe relations, whereas anterior location was considered as dangerous relation [
8]. In contrast, EJV is often considered as a safe and alternate suitable vessel for the therapeutic procedures and monitoring.
Till today, cannulation of external and internal jugular vein is commonly performed by blind techniques using palpable and visual landmarks. The knowledge of the presence and possible variations of jugular veins becomes significant during emergency procedures and operations to avoid inadvertent injury during diagnostic and therapeutic utilization of these veins. Ultrasound guided venipuncture or cannulation should be performed to detect the collateral venous pathways.
Considering the above facts the anomalous communication between the EJV and the IJV cannot be neglected. The presence of such anomalies may be explained in terms of regression and retention of different parts of the veins as found in the monkeys [
9], and may be also as a result of developmental defect. In the present case, the external jugular vein drains that portion of the cephalic venous ring which was incorporated into internal jugular veins. Subsequently, with elongation of the neck, the terminal portion of the external jugular vein moved higher up. Hence, the anterior jugular vein, transverse cervical vein, and suprascapular vein, all of which usually open into the external jugular vein, in the present case opened into the internal jugular vein.
Conclusion
The anomalies described in their current observation presents a unique pattern of congenital renal vascular abnormalities that may be of surgical importance. The knowledge of both normal and abnormal anatomy of the superficial veins of the neck may be important for clinicians performing surgical interventions in this region of the neck.
References
- Standring S. Gray’s Anatomy: The anatomical basis of clinical practice. 39th ed, Churchill Livingstone, New York, 2005; pp. 551.
- Gupta V, Tuli A, Chowdhry R, Agarwal S, Mangal A. Facial vein draining into external jugular vein in humans: its variations, phylogenetic relation and clinical relevance. Surg Radiol Anat. 2003; 25:36-41.
- Lin BS, Kong CW, Tarng DC, Huang TP, Tang GJ. Anatomical variations of the internal jugular vein and its impact on temporary haemodialysis vascular access: an ultrasonographic survey in uraemic patients. Nephrol Dial Transplant. 1998;13:134-138.
- Yadav S, Ghosh SK, Anand C. Variation of superficial veins of head and neck. J Anat Soc India. 2005; 49:61-62.
- Hollinshead WH. Anatomy for surgeons, 3rd ed, Harper and Row, Philadelphia. 1982.
- Deslangiers B, Vaysse P, Combes JM. Contribution to the study of the tributaries and the termination of the external jugular veins. Surg Radiol Anat. 1994;16:173-177.
- Kopuz C, Akan H. The importance of the angulation and termination of external jugular vein in central venous catheterisation in new born. Okajimas Folia Anat Jpn. 1996; 73:155-159.
- Trianos CA, Kuwik RJ, Pasqual JR, Lim AJ. Internal jugular vein and carotid anatomic relations as determined by ultrasonography. Anesthesiology. 1996;85:43-48.
- Robert J. Central venous catheterisation and central venous monitoring. In: Clinical procedures in emergency medicine, 4th edn, Saunders, Philadelphia, 1998; pp. 412-413.