6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffe4e4030000000902000001001000
6go6ckt5b5idvals|239
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Cloacal exstrophy represents the most severe congenital anomaly of the ventral abdominal wall. It is extremely rare entity, with an incidence of 1 in 2.0-4.0 lakh live births [
1]. This complex anomaly is also known by various terminology including: OEIS complex (Omphalocele, exstrophy of cloaca, imperforate anus, spinal defects), vesico-intestinal fissure, exstrophy-epispadias complex. The term OEIS complex was coined by Carey et al [
2]. Various genitourinary, vertebral defects and cardiovascular defects are also known to occur in association with OEIS complex [
3]. We report here a case of OEIS complex managed successfully at our institution.
Case Report
A 2.6 kg male baby born by normal vaginal delivery to a 25 year old mother presents to us for the management of multiple lower abdominal anomalies. Baby was born out of non-consanguineous marriage. There was no significant antenatal history regarding infections, drug or radiation exposure. The baby cried immediately after birth. Baby was hemodynamically stable and there was no respiratory distress or cyanotic spells.
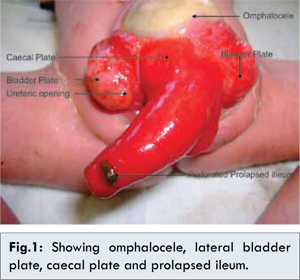
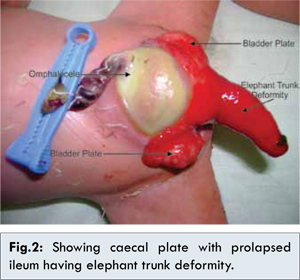
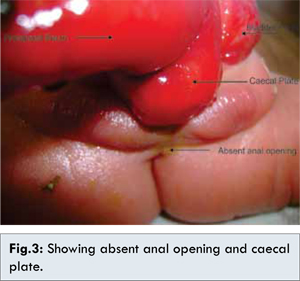
Examination of lower abdomen revealed presence of omphalocele below umbilicus [Fig.1,2]. The central area of the defect was identified as caecal plate with prolapsed terminal ileum with length of about 6-7 cm presenting as characteristic “Elephant trunk deformity” [Fig.2]. There was a small pin hole sized perforation in the prolapsed terminal ileum, which might have occurred during vaginal delivery. On lateral aspects, there were exstrophied bladder plates [Fig.1]. Both ureteric openings were visible with well defined trigone and bladder neck. On caudal aspect baby had small bifid phallus with underdeveloped scrotal folds. No testis could be palpated in the scrotum. Anal opening was absent [Fig.3]. Diagnosis of classical case of cloacal exstrophy with imperforate anus was made.
X-ray examination revealed pelvic diastasis and sacral spinal defects. Ultrasonography abdomen revealed absent right kidney. His complete blood count and renal function tests were within normal limits. No other congenital anomaly was detected on further evaluation.
Baby was resuscitated in intensive care unit and intravenous antibiotics were started. Patient was planned for surgical procedure after extensive counselling of the parents. Both the ureteric orifices were cannulated with 3 Fr. catheters. Both hemi-bladders were mobilized and sutured together in midline, recapitulating the appearance of classic bladder exstrophy [Fig.4]. The omphalocele was reduced to assist abdominal wall closure. The mobilised illeocaecal plate was tubularized along with ileum and brought out as end colostomy. Small rent in the ileum was closed primarily. His renal parameters were within normal range with adequate urine output. His stoma started functioning on 4th post-operative day. Feeds started on 5th day were well tolerated. Patient was discharged on 7th post-operative day and is presently doing well and on regular follow up for definite surgery at 6 months of age.
Discussion
OEIS complex represents a spectrum of congenital malformations ranging in severity from epispadias to bladder exstrophy to cloacal exstrophy. OEIS complex includes omphalocele, exstrophy cloaca, imperforate anus, spinal defects. Cloacal exstrophy is considered the most severe and rare ventral abdominal wall defect among the four components of the OEIS complex.
Embryological explanation for the occurrence of OEIS complex includes the defects of caudal mesodermal migration. This mesodermal migration contributes to the formation of infra-umbilical mesenchyme and invades the cloacal membrane at around 4 weeks of gestation. Simultaneous failure of convergence of cranial, caudal and two lateral body folds results in the defective ventral abdominal wall. Rupture of cloacal membrane before urorectal septum descent results in exposure of exstrophied cloacal membrane. This cloacal exstrophy prevents the development of proctodeum manifesting as anorectal anomalies. This caudal dysgenesis also affects the sacral vertebral development [
4,
5].
A classical case of cloacal exstrophy consists of an infra-umbilical omphalocele superiorly, lateral hemi-bladder plates, ureteric openings inferiorly near trigone and central caecal plate. Ileum may prolapsed from the central caecal plate manifesting as elephant trunk deformity. Male genitalia are usually bifid with pelvic diastasis. Females also have widely spaced labia and bifid clitoris [
6]. Cloacal exstrophy is also associated with other vertebral malformations like scoliosis, kyphosis, sacral agenesis and hemi-vertebrae [
7].
Prenatal diagnosis of OEIS complex is difficult and requires high level of radiologic expertise. Meizner I et al and Noack F et al devised the prenatal diagnostic criteria for OEIS complex [
8,
9]. Major criteria includes non-visualization of urinary bladder, infra-umbilical abdominal wall defect, omphalocele, prolapsed ileum appearing as elephant trunk deformity and myelomeningocoele. Minor criteria are lower extremity defects, genitourinary anomalies and pelvic diastasis.
After delivery and stabilization of the baby, exposed organs and mucosal surface are moistened with warm saline and covered with sterile plastic wrapping to avoid hypothermia and fluid loss. Detailed examination is done to note the sex and size of lateral bladder plates. Karyotyping may be done if gender is not obvious on examination. Patient is managed by multispeciality team comprising of pediatric urologist, pediatric surgeon, pediatric orthopaedic surgeon and pediatric endocrinologist. After complete evaluation, patient is planned for surgery, which should be within 48-72 hours of delivery. The initial surgical procedure consists of separation of intervening caecal plate from lateral bladder plates, closing the omphalocele, bringing out the tubularized caecum as end colostomy and finally closing the bladder or leaving the exstrophied bladder undisturbed for staged closure later.
Our case was a full term vaginally delivered and had classical cloacal exstrophy along with imperforate anus and sacral vertebral defect. On evaluation in our patient, right kidney was absent but renal function was within normal limits. All these finding were consistent with the cases reported in the literature.
Conclusion
OEIS complex is a syndromic entity that was previously thought to be associated with high mortality, but no longer the case presently. Antenatal diagnosis requires skilled sonologist. Important sonographic findings includes non-visualization of bladder, omphalocele, large midline abdominal wall defect and sacral vertebral defects. Management includes initial stabilization and either single stage or multi-staged closure by multi-speciality surgical team. Parental counselling and advice for regular follow up is an integral part of the management protocol.
References
- Hurwitz RS, Manzoni GA, Ransley PG, Stephan FD. Cloacal Exstrophy: A report of 34 cases. Journal of Urology.1987;138:1060.
- Carey JC, Greenbaum B, Hall BD. The OEIS complex (omphalocele, exstrophy, imperforate anus, spinal defects). Birth Defects. 1978;14:253-263.
- Kallen K, Castilla EE, Robert E, Mastroiacovo P, Kallen B. OEIS complex- a population study. Am J Med Genet. 2000;92:62-68.
- Maizels M. Normal and anomalous development of the urinary tract. In: Walsh PC, Retnik AB, Vaughan ED, Wein DJ, (eds). Campbell’s Urology, 7th Edition. Philadelphia. W.B.Saunders Co. 1998: pp.1545-1600.
- Martinez-Frias ML, Bermejo E, Rodriguez-Pinilla E, Frias JL. Exstrophy of cloaca and exstrophy of the bladder: two different expressions of the primary developmental field defect. Am J Med Genet. 2001;99:261-269.
- Ziegler MM, Duckett JW, Howell CG. Cloacal exstrophy. In: Welch KJ, Randolf JG, Ravitch MM, O’Neill JA, Rome MI (eds). Pediatric surgery 4th Edition. Vol 2. Yearbook Medical publishers, Chicago: 1986; pp.764-771.
- Schober JM, Carmichael PA, Hines M, Ramsley PG. The ultimate challenge of cloacal exstrophy. J Urol. 2002;167:300-304.
- Meizner I, Bar-Ziv J. In utero prenatal ultrasonic diagnosis of a rare case of cloacal exstrophy. J Clin Ultrasound. 1985;13:500-502.
- Noack F, Sayk F, Gembruch U. Omphalocele exstrophy imperforate anus-spinal defects complex in dizygotic twins. Fetal Diagn Ther. 2005;20:346-348.