|
|
|
|
|
Fluid Within Striae – An Unusual Phenomenon
|
|
|
pregabalin 150 pregabaline sandoz go Divya Seshadri, Dipankar De, Manish Rathi1, Jane George, Amrinder J Kanwar
From the Department of Dermatology and Department of Nephrology1, PGIMER, Chandigarh, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr. Divya Seshadri
Email: divyaseshadriaiims@gmail.com |
|
|
|
|
|
|
|
|
Received:
9 AUG 2013 |
Accepted:
2-SEP-2013 |
Published Online:
20-SEP-2013 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Striae distensae are common innocuous skin lesions. We report a patient of nephrotic syndrome with corticosteroid-induced large striae, which suddenly developed bulging and fluid accumulation. There were no associated cutaneous or systemic symptoms. Analysis of aspirated fluid showed it was a transudate and culture was sterile. It was concluded that edema fluid, as part of anasarca, had preferentially accumulated within the striae, probably due to their altered dermal mechanical properties. Recognizing this entity is important to avoid unnecessary alarm or irrational use of antibiotics. |
|
|
|
|
|
Keywords :
|
StriaeDistensae, Blister, Edema, Nephrotic syndrome, Antibiotics, Exudates.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff2404040000001802000001000600 6go6ckt5b5idvals|243 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Striae distensae(stretch marks) are very common. They occur naturally during growth spurts, weight gain or pregnancy and can be iatrogenically induced by systemic steroid therapy. We report a patient of nephrotic syndrome who developed sudden progressive bulging of abdominal striae and fluid accumulation within them. To our knowledge, this phenomenon has not been reported earlier.
Case Report
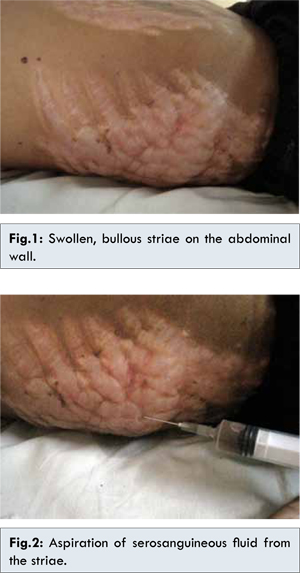
A 14 year old girl was diagnosed to have nephrotic syndrome and started on oral prednisolone 2 mg/kg/day. Few weeks after starting steroid therapy she started developing multiple broad longitudinal striae on the abdominal wall. High dose daily steroids were continued while her nephrotic syndrome followed a fluctuating course and 3 months later she was hospitalized at our institution with ascites and generalized anasarca. During this admission, her abdominal striae were found to be swollen and bulged out. They appeared shiny, translucent and on careful examination, clear fluid could be seen within them [Fig.1]. There was no associated pain, tenderness, itching or erythema or any constitutional symptoms. There was history of discharge of clear fluid from the striae following friction while turning in bed. A kidney biopsy showed mesangioproliferative glomerulonephritis with crescents. The renal function tests (BUN and serum creatinine) were within normal limits while 24-hour urinary albumin was 1.9 grams. Needle aspiration from the swollen striae revealed clear serosanguineous fluid [Fig.2]. On analysis of this fluid, the protein content was 2.2 g/dL. Culture of the fluid was sterile. These findings confirmed that the fluid was a transudate which by definition has protein content below 3 g/dL [ 1]. The serum total protein level was 3.8 g/dL while serum albumin was 1.8 g/dL. It was concluded that edema fluid, as part of generalized anasarca secondary to hypoalbuminemia, had accumulated within the striae.
Discussion
Striae (a.k.a striae distensae or striae atrophicans) are linear atrophic plaques, distributed perpendicularly to the force of greatest tension [ 2]. They are associated with stretching of skin that accompanies rapid increase in size of a particular region; in our patient, high dose steroid therapy as well as anasarca and ascites due to nephrotic syndrome were contributing factors. The histologic analysis of striae reveals collagen fibers that are packed horizontally into thin, straight bundles in contrast with the wavy, thick, and randomly arranged collagen fibersin normal skin. The horizontal stacking of collagen is identical histologically to that of scars [ 3]. On comparing striae with normal skin, a significant reduction in vertical fibrillin fibres subjacent to the dermo-epidermal junction as well as in elastin fibres in the papillary dermis has been demonstrated, along with increased glycosaminoglycan content [ 4].
We propose that the altered dermal mechanics and lowered tensile strength of striae lead to their preferential stretching out by edema fluid and resultant swelling. Moreover, the higher content of glycosaminoglycans, which are hydrophilic molecules, could also produce a selectively greater accumulation of fluid within the striae compared to the surrounding skin. The fact that systemic steroid-induced striae are often larger and broader than physiological striae could have contributed to the dramatic presentation in our patient. To our knowledge, there are no prior reports of this phenomenon. There is one earlier report of Staphylococcal bullous impetigo confined to steroid-induced striae [ 5], but in our patient, clinical and investigative findings revealed no evidence of infection. Interestingly, post-laparoscopic subcutaneous emphysema has been reported along steroid-induced striae, which was attributed to excessive manipulation during surgery and decreased resistance to gas insufflations in striae [ 6].
Subsequently, the authors have encountered other patients with anasarca presenting with bullous fluid accumulation within striae. Such patients are usually admitted in general medicine and allied departments; the alarming appearance often necessitates an urgent dermatology consultation. Both physicians and dermatologists need to be more aware of this entity. The importance of recognizing this phenomenon lies in the fact that needless panic and unnecessary antibiotic therapy can be avoided.
Conclusion
Bullous fluid accumulation within striae is a benign phenomenon with a dramatic presentation that can occur as a part of generalized anasarca.
References
- Kjeldsberg CR, Knight JA (eds). Body fluids: laboratory examination of amniotic, cerebrospinal, seminal, serous & synovial fluids. Chicago, IL: ASCP Press; 1993.
- Yosipovitch G, DeVore A, Dawn A. Obesity and the skin: skin physiology and skin manifestations of obesity. J Am Acad Dermatol. 2007;56:901–916.
- Burk CJ, Pandrangi B, Connelly EA. Picture of the month. Striae. Arch Pediatr Adolesc Med. 2008;162:277-278.
- Watson RE, Parry EJ, Humphries JD, Jones CJ, Polson DW, Kielty CM, et al. Fibrillin microfibrils are reduced in skin exhibiting striae distensae. Br J Dermatol. 1998;138:931–937.
- Bronstein SW, Bickers DR, Lamkin BC. Bullous dermatosis caused by Staphylococcus aureus in locus minoris resistentiae. J Am Acad Dermatol. 1984;10:259–263.
- Nakajima K, Kai Y, Yasumasa K, Nishida T, Ito T, Nezu R. Subcutaneous emphysema along cutaneous striae after laparoscopic surgery: a unique complication. Surg Laparosc Endosc Percutan Tech. 2006;16:119-121.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Seshadri D, De D, Rathi M, George J, Kanwar AJFluid Within Striae – An Unusual Phenomenon.JCR 2013;3:331-333 |
|
Seshadri D, De D, Rathi M, George J, Kanwar AJFluid Within Striae – An Unusual Phenomenon.JCR [serial online] 2013[cited 2026 May 21];3:331-333. Available from: http://www.casereports.in/articles/3/2/Fluid-Within-Striae-An-Unusual-Phenomenon.html |

|
|
|
|
|