6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff84f4030000001e02000001000200
6go6ckt5b5idvals|241
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
When implants are placed first overlooking the planning and patient counseling stage, without the use of surgical templates to guide the positions and angulations of implants, we end up placing less than the required number of implants and always in unfavorable positions and angulations. The seriousness of the problem posed will not be realized till the implants are osseo-integrated and ready for loading. Only after an impression is made and the casts mounted on an articulator will the operator realize that the promised prosthesis cannot be fabricated. When the patient was promised with a fixed denture and it cannot be made, the patient’s hopes are dashed and leads to unwanted misunderstandings.
After explaining the current situation to the patient, if the patient still wants the original treatment plan to be executed, additional implants should be planned. When the patient is opposed to placement of additional implants, the treatment plan can be modified to fabricate an implant and tissue supported removable prosthesis.
Case Report
A 37 year old female patient was referred for prosthetic rehabilitation. On examination the patient was partially edentulous with only four third molars as the remaining natural teeth. Five REPLACE SELECT implants had been placed in the maxillary ridge corresponding to the region of 11, 14, 16, 21 and 25. The mandibular ridge had four EZE HITEC implants corresponding to 35, 36, 45 and 46.
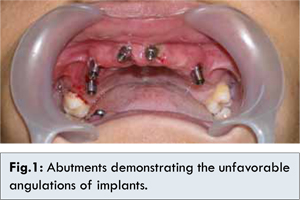
The original treatment plan promised by the implantologist who placed the implant was fixed metal-ceramic prosthesis for the maxillary and the mandibular arch. But this was not possible as the maxillary implants were in prosthetically unfavorable positions and angulations [Fig.1] while the mandibular implants were few in number to support a fixed restoration. A FP-3 type of a fixed prosthesis was planned for the upper jaw [
2-
4]. The possibility of a fixed restoration in the mandibular arch was ruled out as the patient refused to the plan of placement of additional implants. An attachment retained over-denture was hence planned for the lower jaw [
5].
Abutments were secured to the implants in the maxillary arch and the snap-on prosthetic component was fitted to the abutments. This abutment with snap-on acts as the closed tray transfer coping. Ball attachments (Dalabona) were secured to the implants in the mandibular arch. Closed tray impressions were made for both the arches using addition silicone impression material (Aquasil, Densply). The snap-on was picked up in the maxillary impression. Abutments in the maxillary implants were unscrewed and the implant analogs were secured to them. This abutment-implant analogue was repositioned in the maxillary impression by inserting the abutment into the snap-on present in the impression and cast poured. Ball abutment analogue (Dalabona) was positioned in the mandibular impression and cast poured.
Acrylic trial bases were fabricated with relief in the region of implants and a tentative jaw relation was made. The maxillary and mandibular casts were mounted using the tentative record. Castable abutments were secured to the implant analogs in the maxillary cast. The castable abutments were then trimmed to achieve relative parallelism and were joined together in a custom bar wax-up. The wax-up was invested and cast to obtain a bar. This bar was then sectioned into four pieces. The individual pieces were secured to the implants in-vivo and joined together by pattern resin. The bar as a single unit was removed and immediately invested to cast-join the cut pieces. The fit of the bar was once again verified in the patient.
Modeling wax was now added to the cast-joined bar to fabricate an occlusal rim for the maxillary arch. Metal housing was seated over the ball attachment-analogue in the mandibular cast and an acrylic trial denture base and occlusal rim fabricated for the mandibular arch. Both the occlusal rims were then secured to the implants and abutments in the maxillary and mandibular arches respectively. Definitive jaw relation was now recorded and the casts remounted to this new relationship. Teeth arrangement was completed and try-in verification done.
The dentures were processed using Compression Mold technique. The acrylic dentures were then trimmed and polished. The upper denture was then modified to allow access for hygiene procedures. Nylon ‘O’ rings were inserted into the metal housing in the mandibular denture. The fixed maxillary denture was secured to the implant with abutment screws and the removable lower denture was snap fitted over the ball abutments. Occlusion was checked and patient instructed on oral hygiene procedures [Fig.2].
Discussion
Nothing more has to be said about the importance of planning in such situations where the patient walks in with missing or unrestorable and or periodontaly week teeth and walks out in a few hours with implant supported teeth [
1]. When multiple missing teeth are to be replaced with complex prosthesis supported by numerous implants, the treatment has to be executed in three stages. The stages include (i) Planning and Patient counseling, (ii) Implant placement and finally (iii) Prosthetic Rehabilitation. With the availability of planning software and CADCAM technology, patient’s maxilla and mandible can be viewed in three dimension and implant number, location and angulation can be planned [
1]. Surgical templates can be fabricated to place implants in their planned location accurately. CADCAM technology can also mill a temporary prosthesis to be cemented immediately after implant placement. The cost of this technology is often a deterrent and alternative methods are employed to plan.
Surgically driven implant placement without prior planning created a situation of unfavorably positioned and unfavorably angulated implants in the maxillary jaw and inadequate implants in the mandibular jaw for replacement with a fixed prosthesis. Though the patient wanted fixed metal-ceramic bridges for both the arches, the patient was convinced with the new treatment plan of fixed FP3 type of acrylic prosthesis for the maxillary arch and a removable attachment retained denture for the lower jaw. Since the varyingly angulated abutments in the maxillary jaw can be engaged only with a custom made abutment, a cast bar abutment was fabricated and was incorporated in an acrylic, implant supported, fixed denture for the maxillary jaw. The mandibular jaw had inadequate implants to fully support the mandibular prosthesis and so an implant-tissue supported prosthesis was fabricated. Ball abutments were secured to the implants in the mandibular jaw and the implant-tissue supported acrylic denture was made to engage the ball abutments with a nylon “O” ring.
Conclusion
Poor planning had complicated prosthetic rehabilitation. Hence the treatment plan was altered and a logically possible solution was executed after patient counseling. The problem of unfavorable angulation and location was managed by using custom made abutments and the problem of inadequate implants was managed with an implant and tissue supported prosthesis.
References
- Spector L. Computer-aided dental implant planning. Dent Clin North Am. 2008;52:761-775.
- Misch CE. Prosthetic options in Implant Dentistry, In: Misch CE. Contemporary Implant Dentistry. Mosby: St Louis; 1993. pp.43-50.
- Misch CE. Prosthodontic options for implant dentistry. Dent Today. 1989;8:39-44.
- Misch CE. Prosthodontic options in implant dentistry, Int J Oral Implant. 1991;7:17-21.
- Vasant R, Vasant MK. Retention systems for implant-retained overdentures, Dent Update. 2013;40:28-31.