6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffdcbd030000000702000001000b00
6go6ckt5b5idvals|230
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Transverse vaginal septum (TVS) is a rare, autosomal recessive inherited anomaly which develops due to horizontal “wall” of tissue, formed due to partial failure of canalization of either urogenital or mullerian component of the vagina [
1,
2]. TVS can be perforate or imperforate and can develop at nearly all levels in vagina. Commonest positions of TVS are superior vagina (46%), mid vagina (40%), and inferior vagina (14%). Aetiology may lie locally in vaginal mesoderm or in the lack of canalization of the epithelial vaginal plate. We report a 29 year old nulligravida having recurrent cicatrization of transverse vag
inal septum.
Case Report
A 29 years old nulligravida female presented with complains of secondary amenorrhea since last one year with cyclical abdominal pain and abdominal mass since 6 months. She had past history of vaginal surgery at age of 16 years for primary amenorrhea secondary to transverse vaginal septum. She established regular menses for 3 months followed by secondary amenorrhea. After 1 year, she was operated abdominally by transverse incision and she resumed menstruation regularly for one and half years. She underwent dilatation of transverse vaginal septum several times to drain the hematometra and hematocolpos. Eventually, fibrosis of the septum led to secondary amenorrhea. At age of 27 years, she developed intraperitoneal abscess, diagnosed by CT scan for which she was operated abdominally with vertical incision. Intraoperatively, she had dense adhesions of uterus and omentum, hematosalpinx and hematometra and 300 ml pus was drained out. Excision of vaginal septum excision was done.
She presented to us with per abdomen findings of multiple scars of laparotomy. Uterus was enlarged to approximately 24 weeks size with little deviation to right side. Per speculum examination showed TVS with fibrosis. Cervix was not visualized. Per vaginal examination showed blind vagina with approximate length of 3 cm. A mass was felt on per rectal examination. Ultrasound pelvis revealed collection in uterus (10 x 8 cm) and upper vagina (4 x 3 cm) suggestive of hematometra & hematocolpos.
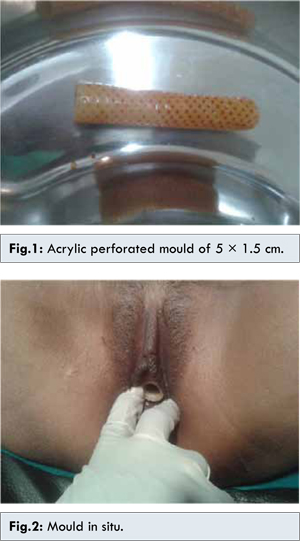
Patient was scheduled for excision of cicatrized vaginal septum by vaginal approach with all pre-operative preparations. Transverse incision of 1 cm was kept between two vaginal dimples. Fibrous tissue of septum was identified and excised circularly. Approximately 1 liter of collected blood was drained. Cervix was identified and sounding was done. Upper and lower vaginal anastomosis was done with interrupted stitches by overlapping technique with Vicryl No.1. A syringe of 10 cc was used as a drain. The nozzle was cut to make a wide opening and edges were blunted. It was kept in vagina for 7 days. After 7 days, syringe was removed and an acrylic mould of 5 × 1.5 cm was kept in vagina under short general anesthesia. Patient was discharged on 10th post-operative day with advice to use mould with aseptic precautions on daily basis and regular intercourse. On one month follow up, patient gave history of normal menstruation for 3 days. On per speculum examination, smooth vaginal mucosa had healed properly with vaginal length of 6 cm. Cervix was well visualized.
Discussion
Transverse vaginal septum is a rare congenital mullerian variety that presents with primary amenorrhea with cyclical abdominal pain. Surgery is always needed to allow normal menstrual blood flow, prevention of dyspareunia and fertility gain. The options for surgical repair depend on the thickness and position of the septa.
The treatment consists of simple excision, Z-plasty techniques and various flaps. Surgical approach for correction involves resection of entire septum and re-anastomosis of upper and lower vagina. Reattachment can easily be accomplished by series of interrupted radial sutures at the site of resection for thin septum. However, mobilisation of usually distended upper vaginal cuff may be necessary to bridge the defect for thick septum. Alternatively preoperative dilatation of septum can be done using menstrual suppression to gain the necessary time to stretch the tissue [
4]. Technique of Z-plasty also reduces the chances of cicatrization [
5]. The danger of a cicatrix forming after excision of the septum requires repeated surgery. Complete resection of transverse vaginal septum with vaginal mucosal anastomosis with overlapping sutures and proper use of vaginal mould can help prevent recurrent fibrosis.
Our patient presented with a recurrent cicatrization of transverse vaginal septum. The major diagnostic challenge in this case was recurrent cicatrization secondary to repeated surgeries and multiple dilatations. Treatment of this case was done by resection of entire septum with anastomosis of upper and lower vagina. Drainage was done with the help of 10 cc syringe by cutting its nozzle and subsequently acrylic mould was used to keep vagina dilated.
Conclusion
To treat a case of transverse vaginal septum needs great expertise, as incomplete resection of septum can put the patient at risk of repeated surgeries. Complete resection of septum by identifying the extent of cicatrisation and reunion of upper and lower vagina by overlapping sutures can out risk the patient from repeated failures. Z plasty technique or use of various flap techniques is the good alternatives. Regular use of mould post operatively is must for such cases.
References
- Elyan A, Saeed M. Mullerian duct anomalies: Clinical concepts. ASJOG. 2004;1:11-20.
- Joe Leigh Simpson. Genital Duct Anomalies. Glob. Libr. Women’s Med. 2012 DOI 10.3843/GLOWM.10359.
- Gidwani G, Falcone T. Congenital malformations of the female genital tract. Diagnosis and management; Philadelphia: Lippincott Williams & Wilkins; 1999. pp. 145–168.
- Harold P. Drutz, Sender Herschorn, Nicholas E. Diamant (eds). Female Pelvic Medicine and Reconstructive Pelvic Surgery. Springer: London;2003.
- Polasek PM. Transverse vaginal septum associated with tubal atresia; Mayo Clin Proc. 1995;70:965-968.