|
|
|
|
|
A Rare Case of Carcinoma of Ovary with Carcinoma of Cervix
|
|
|
RD Katke, Shruti Gadekar, Priyanka Pagare
From the Department of Obstetrics & Gynecology, Grant Government Medical College & Sir J. J. Group of Hospitals, Mumbai, Maharashtra, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Rajshree D. Katke
Email: drrajshrikatke@gmail.com
|
|
|
|
|
|
|
|
|
Received:
06-APR-2014 |
Accepted:
03-JUN-2014 |
Published Online:
25-JUN-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Synchronous malignancies of cervix and ovary are rare with poor prognosis and are found in the literature only as case reports. The optimal management remains poorly defined. We present a case of carcinoma ovary with carcinoma cervix that was treated with Wertheim’s hysterectomy with pelvic lymph node dissection and omentectomy. Her postoperative period was uneventful. A successful outcome was obtained and patient could go back to her normal life and work.
|
|
|
|
|
|
Keywords :
|
Hysterectomy, Ovarian Neoplasms, Lymph Node Excision, Uterine Cervical Neoplasms.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff14d105000000e702000001000a00
6go6ckt5b5idvals|332
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Synchronous genital tract malignancies are rare. The most frequently observed synchronous neoplasms are those of the ovary together with the endometrium constituting 40% of all and carries favorable prognosis because of its low malignant potential [1]. Overall incidence of synchronous female genital tract malignancies is 0.63% [2,3]. Cervical and ovarian malignancies are still rare and if they occur they have similar histopathology due to direct spread of cervical malignancy to ovary. The literature on both the spread of cervical carcinoma and metastatic tumors to the ovary indicates that ovarian involvement by cervical carcinoma is rare if cases of direct spread are excluded. An important category of cervical carcinomas that may show ovarian spread is adenocarcinoma and related tumors, including adenosquamous carcinoma and glassy cell carcinoma [4]. We are presenting a rare case report of synchronous squamous cell carcinoma of cervix and serous papillary cyst-adenocarcinoma of ovary.
Case Report
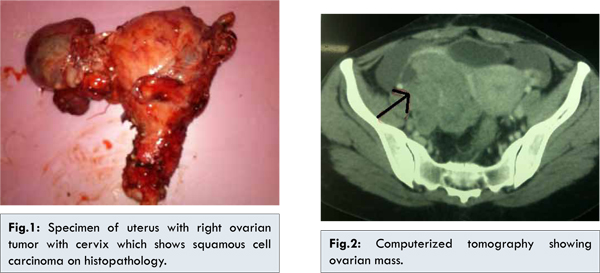
A 40 year female with foul smelling discharge per vaginum and postcoital bleeding since 3 months was referred to us. She was diagnosed as a case of ovarian malignancy with moderately differentiated squamous cell carcinoma of cervix, histopathologically proved on cervical biopsy. Her Tumor marker cancer antigen were evaluated and CA-125 was found to be raised (CA 125: 774 U/mL); whereas other tumor markers were normal [Alpha fetoprotein (AFP) was 3.37 ng/mL, ß HCG < 1.2 IU/mL, CA 19.9 < 2 IU/mL, LDH: 320U/L]. Fine needle aspiration cytology (FNAC) of right ovarian mass was suggestive of carcinoma; whereas cervical biopsy showed presence of squamous cell carcinoma. Per abdomen examination revealed solid, non-mobile palpable mass of approximately 8x8x7 cm arising from pelvis. On per speculum examination cervical erosion, hypertrophied cervix and biopsy mark were noted. After getting anesthetic fitness patient was posted for surgery. In situ findings revealed ascites, 15x10x10 cm necrotic hemorrhagic, cystic, friable tumor mass arising from right ovary. Mass was adherent to rectum and adjacent pelvic structures. It was separated from bowel and surrounding structures by blunt and sharp dissection. Total abdominal hysterectomy with removal of right sided ovarian tumor with left sided salpingo-oophorectomy with bilateral internal iliac, external iliac, obturator and para-aortic lymph nodes dissection and omentectomy was done. Uterus, tumor mass, cervix with dissected lymph nodes were sent for histopathological examination [Fig.1]. Vault closure was done with vicryl number 1 continuous interlocking suture. After achieving complete hemostasis abdomen was closed in layers.
Patient withstood the procedure well. Postoperative period of patient was uneventful. Stich removal was done on day 11. Histopathology report revealed squamous cell carcinoma of cervix and high grade serous papillary cystadenocarcinoma of ovary [Fig.3,4]. Chemotherapy was given to the patient post-operatively and patient is on regular follow-up.
Discussion
Simultaneous occurring genital tract malignancies can be synchronous or metachronous. Primary malignancies of the genital tract seem to occur synchronously more often than one would expect as it was seen in our case [5]. The prognoses in both the groups differs; those with synchronous malignancies have better prognosis when compared to metastatic lesions of individual tumors [6,7]. While the etiology of this phenomenon remains unclear, it has been postulated that embryologically similar tissues of the female genital tract, when simultaneously subjected to carcinogen may develop synchronous neoplasm. These neoplasms may represent metaplasia.
Functional exact Swiss Replica Rolex Watches UK on amazon with high quality for men - Rolex, TAG Heuer and Breitling.
Buying luxury replica watches ca with both low price and high quality at our online store.
Incidence of synchronous genital tract malignancy is 0.63%. Out of this endometrioid carcinoma of ovary and endometrium constitutes 40% [2]. Literature shows very few case reports on synchronous cervical and ovarian malignancy. Earlier reported cases were of ovarian endometrioid adenocarcinoma and frank squamous cell carcinoma of cervix in 1996 by Jawornik and colleagues [8]. Only one similar case with ovarian cyst-adenocarcinoma and squamous cell carcinoma of cervix has been reported by K.Srivastav and colleagues in 2009 [2]. In 2006, Huang YD and colleagues reported ovarian endometrioid adenocarcinoma and endocervical mucinous adenocarcinoma [9]. Our patient had squamous cell carcinoma of cervix along with high grade ovarian serous cysadenocarcinoma. While these cases represent synchronous involvement, a case study conducted by Elishaev E showed that endocervical adenocarcinomas, including some qualifying as microinvasive, can metastasize to the ovaries and simulate primary ovarian surface epithelial neoplasms [10]. The literature on both the spread of cervical carcinoma and metastatic tumors to the ovary indicates that ovarian involvement by cervical carcinoma is rare if cases of direct spread are excluded. An important category of cervical carcinomas that may show ovarian spread is adenocarcinoma and related tumors, including adenosquamous carcinoma and glassy cell carcinoma [11]. HPV staining may be used in demonstrating metastatic involvement on ovary by cervical malignancy.
Based on our case report we need to keep in mind that even if patient presents with symptoms pertaining to a single malignancy; still the rare possibility of synchronous malignancies should be looked for by doing proper investigations. In our case, patient had symptoms pertaining to cervical malignancy; whereas ovarian malignancy was diagnosed after investigating the patient. Histologic examination should be done properly as the prognosis depends on the malignancies being metastatic or synchronous ones; the latter group having better prognosis as shown by earlier studies [2,8,9]. Surgical management should be offered in all such cases as it greatly aids in diagnosis and also helps in improving overall survival. Long term follow up of such patients should be maintained to determine the prognosis.
References
- Ayhan A, Yalçin OT, Tuncer ZS, Gürgan T, Küçükali T. Synchronous primary malignancies of the female genital tract. Eur J Obstet Gynecol Reprod Biol. 1992;45(1):63-66.
- Srivastava K, Zahra F. Synchronous primary malignancy of ovary and cervix with different histopathology: a rare presentation. The Internet Journal of Gynecology and Obstetrics 2009; Volume 12 Number 2.
- Kambi DP, Mallikarjuna M, Santosh C, Abhishek V. Synchronous malignancies of ovary, fallopian tube and cervix: A rare case. International Journal of Biomedical and Advance Research 2013;4(9):676-679.
- Young RH, Gersell DJ, Roth LM, Scully RE. Ovarian Metastases from Cervical Carcinomas Other than Pure Adenocarcinomas. Cancer J 1993;71(2):407-416.
- Desai R, Darad D, Chugh A, Patel H. A case report of 2 synchronous tumors of female genital tract – rare finding. National journal of Medical Research 2012;2(1):102.
- Matloch DL, Salem FA, Charles EH, Save EW. Synchronous multiple primary neoplasms of the upper female genital tract. Gynec Oncol 1982;13:271.
- Eifel P, Henricksen M, Ross W, Ballon S, Martines A, Kempson R. Simultaneous presentation of carcinoma involving the ovary and the uterine corpus. Cancer 1982;50:163.
- Pitynski K, Bogdanowicz M, Jawornik M. Coexistence of endometrioid ovarian tumor and squamous cell carcinoma of the cervix. Ginekol Pol 1996;67(12):629-631.
- Huang YD, Hung YC, Yeh LS, Chiang IP, Zeng GC, Chang WC. Synchronous ovarian endometrioid adenocarcinoma and endocervical mucinous adenocarcinoma. Taiwan J Obstet Gynecol. 2006;45(3):264-267.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Katke RD, Gadekar S, Pagare PA Rare Case of Carcinoma of Ovary with Carcinoma of Cervix.JCR 2014;4:217-220 |
|
Katke RD, Gadekar S, Pagare PA Rare Case of Carcinoma of Ovary with Carcinoma of Cervix.JCR [serial online] 2014[cited 2026 Jul 14];4:217-220. Available from: https://www.casereports.in/articles/4/1/A-Rare-Case-of-Carcinoma-of-Ovary-with-Carcinoma-of-Cervix.html |

|
|
|
|
|