6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff04aa05000000a902000001000500
6go6ckt5b5idvals|304
6go6ckt5b5|2000F757Tab_Articles|Fulltext
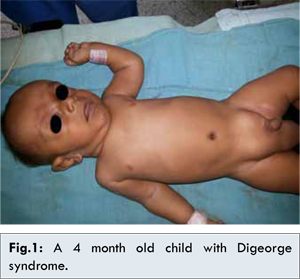
A 4 month old male child weighing 4.5 kg presented to us for emergency exploration for obstructed right inguinal hernia [Fig.1]. General physical examination showed that the child had abnormal facies and cleft palate. Systemic examination revealed pan systolic murmur on chest auscultation. Respiratory system was normal. Birth history revealed that the child was normal full term vaginal delivery born to non-consanguineous parents. Child was ventilated for 24 hours in view of birth asphyxia. At one month of age he developed sudden breathlessness for which he was hospitalized and treated. Echocardiography done at that time reported severe tricuspid regurgitation and small patent ductus arteriosus with right to left shunt. Preoperatively patient was investigated. Parathormone levels were 10 pg/mL (normal level: 11-54 pg/mL) and calcium levels were 7.1 mg/dL (normal: 9-11 mg/dL). Hematological investigations were within normal limits. All these clinical features and investigation parameters lead us to suspect Digeorge syndrome in this child.
Patient was premedicated with syrup midazolam half hour prior to surgery. Injection calcium gluconate was given slowly under cardiac monitoring. Anesthesia was induced with injection glycopyrrolate (0.04 mg) and ketamine (2 mg/kg). Caudal block was performed using 4.5 mL, 0.2% ropivacaine with injection clonidine 1 µg/kg as adjuvant. Patient was kept on mask breathing spontaneously through Jackson Rees circuit and was maintained on 50% oxygen and 50% air along with titrated propofol infusion. Intraoperative and post-operative period was uneventful with stable vitals.
Digeorge syndrome is caused due to deletion within chromosome 22q11. It is also known as CATCH22 syndrome. C: Cardiac defect, A: Abnormal facies, T: Thymic hypoplasia, C: Cleft palate and H: Hypocalcemia. In our patient, all these features were present. Digeorge described this syndrome in 1956 in a child with recurrent infections and hypoparathyroidism [1].
There are very few cases in literature describing anesthetic management of Digeorge syndrome [2,3]. For anesthesiologist it is important to know problems associated with this syndrome. These patients have craniofacial dysmorphism and may have difficult airway due to cleft palate and short trachea [4]. Also there is risk of hypocalcemic seizures while recovering [3]. If serum ionized calcium levels are low, patient should be supplemented with intravenous calcium and vitamin D therapy, because hyperventilation and subsequent alkalosis further decreases serum ionized calcium resulting in seizures which may be masked due to muscle relaxants intra operatively but become evident during recovery. Hence, regional anesthesia is preferred over general anesthesia with muscle relaxants whenever feasible in these patients. Although blood transfusion was not needed in our case but in any case rapid transfusion of blood can lead to chelation of calcium by citrate and decrease in serum ionized calcium levels [5].
Hence, patients of Digeorge syndrome should be evaluated for hypocalcemia, cardiovascular anomalies and difficult airway. We successfully managed our case of obstructed inguinal hernia with caudal analgesia and sedation.
References
- Cooper MD, Peterson RDA, Good RA. A new concept of the cellular bases of immunity. J Pediatr. 1956;67:907-908.
- Ji-Young Lee, Yun-Joung Han Korean. J Anesthesiol. 2011;60(6):449-452.
- Michael H. Flashburg, Burdett S. Dunbar. Anesthesiology. 1983;58:479-480.
- Singh VP, Agarwal RC, Sanyal S, Waghary MR, Luthera MI, Brocar JM. Anesthesia for Digeorge’s syndrome. J Cardiothoracic Vascular Anesthesia. 1997;11:811.
- Khan RC, Jascott D, Carlon GC, Schweitzer O, Howland WS, Goldenger PL. Correlation of ionized calcium, citrate, and hydrogen ion concentration. Anesth Analg (Cleve). 1979;58:278.