|
|
|
|
|
Inflammatory Pseudotumor of Perirenal Soft Tissue
|
|
|
Pramod S, Shirish Mishra, Girish Nelvigi , CR Ratkal, CR Chandrashekar
From the Department of Urology, Institute of Nephrourology, Bangalore, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Pramod S
Email: meetdr.pramod@gmail.com
|
|
|
|
|
|
|
|
|
Received:
10-DEC-2013 |
Accepted:
28-MAR-2014 |
Published Online:
05-MAY-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Inflammatory pseudotumor or inflammatory myofibroblastic tumor (IMT) of kidney or perirenal soft tissue is rare benign lesion of unknown etiology, seen mostly in children and young adults. Less than forty cases have been found in the kidney, and less than five cases have been reported in the perirenal tissue. This tumor has been misdiagnosed by pathologists as myxoid leiomyosarcomas, and sarcomatoid carcinomas of kidney in the past. Immunohistochemistry is the key for the diagnosis and urologists should make their pathologists aware of the existence of such condition so that postoperatively benign nature of the condition and good prognosis can be explained to the patient.
|
|
|
|
|
|
Keywords :
|
Carcinoma, Neoplasms, Leiomyosarcoma, Granuloma, Plasma Cell.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff90c1050000002602000001000b00 6go6ckt5b5idvals|314 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Inflammatory pseudotumor or inflammatory myofibroblastic tumor (IMT) of kidney or perirenal soft tissue is rare benign lesion of unknown etiology, seen mostly in children and young adults.Less than forty cases have been found in the kidney, and less than five cases have been reported in the perirenal tissue. We describe a young male patient with inflammatory pseudotumor of right perirenal tissue.
Case Report
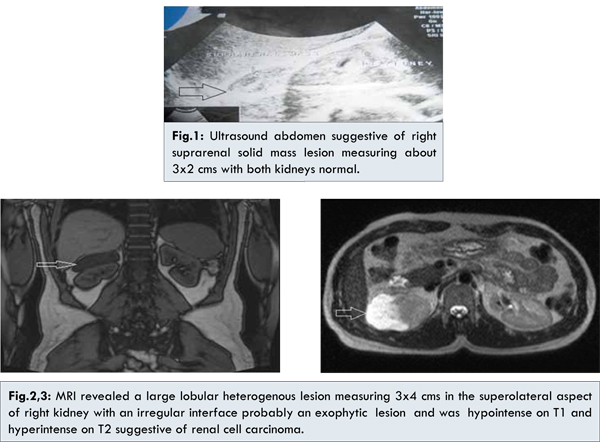
A 29 year old male presented with right loin pain for 6 months which was dull, continuous and non-radiating. There was no history of fever, hematuria, loss of weight or appetite and urinary tract symptoms. He was a non-smoker and farmer by occupation. Physical examination was unremarkable. Biochemical and hematological investigations were unremarkable. X-ray KUB was inconclusive. Ultrasound abdomen was performed, which revealed a 3x2 cm right suprarenal solid mass lesion with no evidence of renal involvement [Fig.1].MRI revealed a large lobular heterogenous lesion measuring 3x4 cms in the superolateral aspect of right kidney with an irregular interface probably an exophytic lesion which was hypointense on T1 and hyperintense on T2 suggestive of renal cell carcinoma [Fig.2,3]. In view of negative metastatic work up, right partial nephrectomy was planned.
Intraoperatively, there was a well circumscribed lesion in right superolateral aspect of right kidney in perirenal tissue and showed no infiltration into the renal tissue [Fig.4]. Therefore enucleation of lesion was done. Microscopy showed bland appearing spindle cells in fibromyxoid stroma, lymphocytic infiltration, absence of mitotic figures [Fig.5]. Immunohistochemistry showed desmin and vimentin positivity and negative for ALK, CD99, and CD 34 [Fig.6] and diagnosed as inflammatory pseudotumour of perirenal soft tissue.
Discussion
Inflammatory myofibroblastic tumor (IMT) is known by several names, including inflammatory pseudotumor, pseudo-sarcomatous, fibro-myxoid tumor, fibrous xanthoma and plasma cell granuloma. IMT is a rare entity with distinctive histologic features. Originally described in the lung, IMT has now been reported at multiple extrapulmonary sites. In the urogenital tract, the bladder is the most frequently involved organ. Less than forty cases have been found in the kidney, and less than five cases have been reported in the perirenal tissue [1]. The IMT and similar tumors were first seen in the lungs and published by Brunn et al in 1939 [2,3]. Roth was the first who reported a pseudosarcomatous tumor in the bladder in 1980 [4].
Patients usually present with hematuria and/or abdominal pain. Clinical examination and radiological investigations are often inconclusive.Our case is unique because our patient presented with dull aching right flank pain since 6 months with no symptoms of hematuria. Our patient was presumed to have renal cell carcinoma in view of MRI findings. The surprise morphological finding of discrete swelling in the perirenal area near the upper pole of right kidney and normal adjacent adrenal tissue raised the possibility that this may a benign tumor. This was confirmed histologically.
Histologically, they consist of proliferation of spindle cells admixed with various amounts of lymphocytic-plasmacytic infiltrate, spindle cell proliferation and absence of significant necrosis, cytologic atypia and abnormal mitotic figures.
Because IMT can be confused with both reactive processes as well as potentially malignant neoplasm, distinguishing them from their histologic mimics plays an important role in assuring appropriate patient management. Three histologic patterns (myxoid-vascular pattern, compact spindle cell pattern, and hypocellular fibrous pattern) of IMT have been described by Coffin et al [5]. Immunohistochemical studies support the myofibroblastic nature of this lesion with consistent expression of vimentin and smooth muscle actin. Variable positivity has been identified for HHF-35, cytokeratins, and CD68.
Studies have identified clonal abnormalities in the short arm of chromosome 2 in the region of p21-23 in myofibroblastic tumors, the site of the ALK gene that codes for a tyrosine kinase receptor [7]. ALK-positive cases tend to occur in children and young adults, and ALK-negative cases tend to occur in older patients.
Due to the marked inflammatory pattern, infectious and autoimmune etiologies have been suspected for the pathogenesis of IMT. Some microbiological agents and autoimmune diseases were blamed, but clear etiology could not be determined. A variety of infectious agents including Actinomyces, Pseudomonas species, and Mycoplasma have been associated with IMT. Another suggested etiologic agent is Epstein-Barr virus, as some cases of IMT have been positive for Epstein-Barr virus latent membrane protein, especially in the liver and spleen [8-10].
Treatment of renal and perirenal IMTs is almost exclusively by means of surgery and nephrectomy and partial nephrectomy have been done for renal IMT whereas perinephric IMT have been treated with enucleation because the presentation of these masses usually is indistinguishable from other renal lesions. High dose corticosteroid therapy (1 mg/kg) has been attempted in 3 patients [11].
Conclusion
This tumor has been misdiagnosed by pathologists as myxoid leiomyosarcomas, and sarcomatoid carcinomas of kidney in the past. Immunohistochemistry is the key for the diagnosis and urologists should make their pathologists aware of the existence of such condition so that postoperatively benign nature of the condition and good prognosis can be explained to the patient.
References
- Sibel Bektasa, Emrah Okuluc, Onder Kayigilc, Dilek Ertoy Baydara. Inflammatory myofibroblastic tumor of the perirenal soft tissue misdiagnosed as renal cell carcinoma. Pathology – Research and Practice 2007; 203:461–465.
- Lakshmana Das Narla, Beverley Newman, Stephanie S. Spottswood, Shireesha Narla, Rajasekhar Kolli. Inflammatory pseudotumor: Radiographics. 2003;23:719-729.
- Umiker WO, Iverson LC. Post inflammatory tumor of the lung: report of four cases simulating xanthoma, fibroma or plasma cell granuloma. J Thorac Surg.1954;28:55-62.
- Roth JA. Reactive pseudosarcomatous response in urinary bladder. Urology1980;16:635–637.
- Coffin CM, Watterson J, Priest JR. Extra-pulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor). A clinical, pathologic and immunohistochemical study of 84 cases. Am J Surge Pathol.1995;19(8):859–872.
- Griffin CA, Hawkins AL, Dvorak C, Henkle C, Ellingham T, Perlman EJ. Recurrent involvement of 2p23 in inflammatory myofibroblastic tumors. Cancer Res 1999;59:2776–2780.
- Su LD, tayde-Perez A, Sheldon S, Fletcher JA, Weiss SW. Inflammatory myofibroblastic tumor: cytogenetic evidence supporting clonal origin. Mod Pathol.1998;11(4):364-368.
- Arber DA, Kamel OW, van de Rijn M, Davis RE, Medeiros LJ, Jaffe ES, et al. Frequent presence of the Epstein-Barr virus in inflammatory pseudotumor. Hum Pathol. 1995;26:1093–1098.
- Brittig F, Ajtay E, Jakso P, Kelenyi G. Follicular dendritic reticulum cell tumor mimicking inflammatory pseudotumor of the spleen. Pathol Oncol Res. 2004;10:57–60.
- Babu S, Singhai A, Hussain N, Singh V. Renal Leiomyosarcoma – A Rare Entity. Journal of Case Reports. 2014;4(1);29-32.
- Li JY, Yong TY, Coleman M, Astill D, Passaris G, Juneja R, et al. Bilateral renal inflammatory pseudotumor effectively treated with corticosteroid. Clin Exp Nephrol. 2010;14:190–198.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
S Pramod, Mishra S, Nelvigi G, Ratkal CR, Chandrashekar CRInflammatory Pseudotumor of Perirenal Soft Tissue.JCR 2014;4:147-150 |
|
S Pramod, Mishra S, Nelvigi G, Ratkal CR, Chandrashekar CRInflammatory Pseudotumor of Perirenal Soft Tissue.JCR [serial online] 2014[cited 2026 Jun 6];4:147-150. Available from: https://www.casereports.in/articles/4/1/Inflammatory-Pseudotumor-of-Perirenal-Soft-Tissue.html |

|
|
|
|
|