|
|
|
|
|
Minimally Invasive Endoscopic Surgical Repair of Recurrent Complete Third Branchial Fistula in a Nine Year Old Girl
|
|
|
Sanjeev Mohanty, M. Gopinath
Department of ENT, Head and Neck Surgery, Sri Ramachandra University, Porur, Chennai- 600116, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Sanjeev Mohanty
Email: drsanjeevmohanty@gmail.com
|
|
|
|
|
|
|
|
|
Received:
19-APR-2014 |
Accepted:
22-MAY-2014 |
Published Online:
20-JUN-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Congenital anomalies of the branchial arches are well known with fistulas presenting in the head and neck region. A proper diagnosis of this uncommon entity is mandatory for a successful surgical repair in the first attempt itself. In this case report, we profile a patient who was subjected to multiple surgeries only to result in subsequent breakdowns and resurfacing of symptoms. An innovative attempt was made with the use of endoscopes and minimally invasive surgical methods to repair this recurrent fistula and followed up with a repeat fistulogram which showed a complete closure of the tract without any co-morbidity.
|
|
|
|
|
|
Keywords :
|
Fistula, Endoscopy, Pyriform Sinus, Neck, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff5cc905000000dd02000001000f00 6go6ckt5b5idvals|331 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
A complete congenital
fistula of the 3rd branchial apparatus is a rare clinical occurrence.
The branchial arches and its anomalies have been well described and held
accountable for many of the symptomatology in the head and neck region,
especially in children. They may present with recurrent infections in
the neck, supra-tonsillar fossa and the pyriform sinuses. There are
various modalities of surgical treatment which includes the standard
step ladder excision of extensive fistulas and the innovations in
minimally invasive surgical repair methods. In a patient presenting with
unsuccessful surgical attempts to repair, a careful treatment planning
is required to prevent any further leaks. This patient was subjected to
an innovative minimally invasive surgical method to strip the tract
completely and carefully address the internal opening to set aside any
chance of recurrence in future.
Case Report
A nine
year old child presented to the ENT clinic, with history of discharging
sinuses on and off, on the left side of neck of 6 years duration.
Although she was comfortable with taking solid food, a very significant
history of fluid leak was present during an act of swallowing fluids
through the opening. She had undergone unsuccessful surgical repair for
the same ailment three times in the past. Intermittently, she exhibited
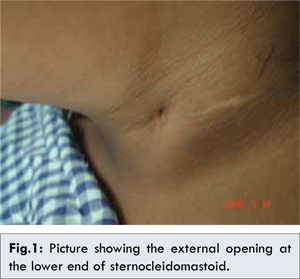
signs of inflammation along with discharge at the same site. On
examination, the external opening of the fistulous tract was detected at
the junction of the middle and lower third of the anterior border of
the sternocleidomastoid muscle on the left side [Fig.1].
On
giving a test feed, fluid leaked out of the same site only during the
act of swallowing. She was subjected to radiological investigations
after an unremarkable hematological laboratory values. Fistulogram was
performed after cannulating the external opening and injecting contrast
material. The entire fistulous tract was delineated and the dye was seen
entering the hypopharynx at the medial wall of the left pyriform sinus
[Fig.2,3]. A clinical diagnosis of left recurrent complete branchial
fistula was made.
Exploration and excision of the fistulous tract
was planned under general anaesthesia. A combined approach was
undertaken, with an external and endoscopic access to reach out to the
tract from inside and outside simultaneously. A transverse elliptical
incision was made and the external opening was delineated by careful
dissection of the tract from the surrounding tissues [Fig.4].
Using a
minimally invasive video assisted endoscopic approach, the internal
opening was visualized on the medial wall of the left pyriform fossa
[Fig.5]. With the additional help of the suspension laryngoscopy and use
of microlaryngeal instruments 3.0 vicryl was railroaded and needled
through the internal opening and the tract was marsupialised completely.
The entire fistulous tract was excised. Histopathological examination
of the excised clinical specimen revealed pseudo-stratified ciliated
columnar epithelium lined structure with lymphoid follicles in keeping
with the diagnosis of branchial fistula.
After a brief stay in
hospital, she was discharged in a very stable condition without any
co-morbidity. A check fistulogram done 4 weeks post operatively showed
no evidence of any leak from the operated site.
Discussion
The
branchial apparatus comprises of six arches with the mesoderm as its
core, separated by clefts and pouches on the ectoderm and endodermal
sides, respectively [1]. Maldevelopment of the branchial apparatus
leads to anomalies that occur in the form of cysts, sinus or fistulas.
These anomalies may originate from the first to fourth cleft/ pouch,
with the commonest arising from the second cleft/ pouch (95%) [2].
Our
patient had a true fistula with both internal and external openings. A
branchial fistula is thought to form when the mesenchyme that separates
the cleft and pouch involutes, thus uniting them [3]. Therefore, the
fistula would be caudal to the structures derived from the corresponding
arch and dorsal to the structures from the following arch.
Third
branchial arch anomalies are rare. Anatomically, these fistulas have an
external opening in the mid or lower part of the neck along the
anterior border of the sternocleidomastoid muscle. They have a
demonstrable connection with the left pyriform sinus. A third branchial
fistula would course between the third and fourth arch structure. In
theory, the course starts externally from the skin opening at the upper
third of the sternocleidomastoid muscle, through the subplatysmal plane
near (not through!) the superior pole of the thyroid gland, and then
ascends along the carotid sheath posterior to the internal carotid
artery, under the glossopharyngeal nerve (third arch derivative) and
superficial to the hypoglossal nerve (fourth arch derivative). It then
pierces the thyrohyoid membrane, which lies superior to the thyroid
cartilage (fourth arch derivative) and passes above the superior part of
the pyriform fossa [1].
It has been reported that the typical
course of a fistulous tract is not observed in cases of a large mass or
concomitant cyst [4]. Jaka and Singh et al reported a complete third
branchial fistula that followed the famously described tract that passes
posterior to the common and internal carotid artery, but they did not
mention the involvement of the thyroid gland [5]. The course of these
fistulas is not always typical. Edmonds et al. have recommended the use
of direct laryngoscopy and transillumination of the tract with a rigid
telescope [6]. Treatment is to excise the tract completely. Complete
excision of the fistula prevents any recurrence. The recurrence rate of
branchial anomaly is 3% for a primary lesion and as high as 22% for
lesions with previous infection and surgery [7]. It should be borne in
mind that aberrant presentations may exist when re operating on chronic
branchial fistulas.
Conclusion
Congenital branchial
fistulas are infrequently encountered in clinical otolaryngological
practice. However, a complete fistula of the third branchial arch is
relatively rare. This particular case is unique in its presentation as
multiple surgeries were attempted to repair the defect without
addressing the internal opening in the pyriform sinus. This incomplete
excision probably led to recurrence. The depth of the internal opening
in the pyriform sinus made it more challenging per operatively. The use
of microlaryngeal instruments along with the assistance of video
endoscopes helped immensely in sealing the tract completely.
References
- Link TD, Bite U, Kaspebaur JL, Harner SG. Fourth branchial pouch
sinus: a diagnostic challenge. Plastic Reconstructive Surgery
2001;108:695-701.
- Gross E, Sichel JY, Congenital neck lesions. Surgical Clinics of North America 2006;86:383-392.
- Yang C, Cohen J, Everts E, Smith J, Caro J, Andersen P. Fourth
branchial arch sinus: Clinical presentation, diagnostic work up and
surgical treatment. Laryngoscope 1999;109:442-446.
- Liberman M,
Kay S, Emil S, Flageole H, Nguyen LT, Tewfik TL, et al. Ten years of
experience with third and fourth branchial remnants. Journal of
pediatric surgery 2002;37:685-690.
- Jaka RC, Singh G. Complete
congenital third branchial Fistula on the right side. Otolaryngology,
Head Neck Surgery 2007;137:518-519.
- Edmonds JL, Girod DA,
Woodroof JM, Bruegger DE. Third branchial anomalies. Avoiding
recurrences. Archives of Otolaryngology, Head Neck Surgery
1997;123:438-441.
- Choi SS, Zalzal GH, Branchial anomalies; A review of 52 cases. Laryngoscope 1995;105;909-913.
- Miller MB, Cohn AS, Case report: Fourth branchial pouch sinus. Ear, Nose, Throat Journal 1993;72(5):356-358.
- Ng SK, Tong MC, Van Hasselt CA. Second branchial fistula with unusual presentation. Laryngoscope 2010;120(7):1319-1321.
- Yilmazi, Cakmak O, Ozgirgin N, Boyvat F, Dermirhan B. Complete fistula
of the second branchial cleft- case report of Catheter guided total
excision. International Journal of Pediatric otolaryngology
2004;68(8);1109-1113.
- Madana J, Yolmo D, Gopalakrishnan S,
Saxena SK. Complete congenital third arch branchial fistula with left
sided, recurrent, suppurative thyroiditis. Journal of Laryngology and
Otology 2010;124:1025-1029.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Mohanty S, Gopinath M.Minimally Invasive Endoscopic Surgical Repair of Recurrent Complete Third Branchial Fistula in a Nine Year Old Girl.JCR 2014;4:213-216 |
|
Mohanty S, Gopinath M.Minimally Invasive Endoscopic Surgical Repair of Recurrent Complete Third Branchial Fistula in a Nine Year Old Girl.JCR [serial online] 2014[cited 2026 May 27];4:213-216. Available from: http://www.casereports.in/articles/4/1/Minimally-Invasive-Endoscopic-Surgical-Repair-of-Recurrent-Complete-Third-Branchial-Fistula-in-a-Nine-Year-Old-Girl.html |

|
|
|
|
|