|
|
|
|
|
Mucocele of Appendix Vermiformis due to Mucinous Cystadenoma with Carcinoma in Situ Component
|
|
|
benadryl and pregnancy second trimester benadryl and pregnancy
Department of General Surgery1, Pathology2 and Emergency Medicine3; Dumlupinar University, Faculty of Medicine, Kutahya, Turkey. |
|
|
|
|
|
Corresponding Author:
|
Dr. Zulfu BAYHAN
Email: zulfubayhan@gmail.com
|
|
|
|
|
|
|
|
|
Received:
16-FEB-2014 |
Accepted:
30-APR-2014 |
Published Online:
20-MAY-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Acute appendicitis is one of the most common clinical presentations among the patients with acute abdominal pain. However, a through clinical and surgical evaluation is essential to manage atypical conditions such as carcinoids and the tumors of appendix or mucocele appendix. Here, we present a case with mucocele of appendix vermiformis due to mucinous cystadenoma with carcinoma in situ component. This case indicates that atypical presentations and clinical findings should be carefully managed in the patients with suspicious acute appendicitis in surgery. This is especially essential in the patients with appendiceal mass or mucocele in order to minimize complications.
|
|
|
|
|
|
Keywords :
|
Abdominal Pain, Appendicitis, Cystadenoma, Mucinous Adenocarcinoma, Carcinoid Tumor.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa4c105000000e502000001000f00 6go6ckt5b5idvals|319 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Acute appendicitis is one of the most common diagnosis in the patients with acute abdominal pain and requires immediate surgical intervention. Luminal obstruction is the primary pathophysiological mechanism in the development of inflammation in the appendix vermiformis [1]. Surgery, either with laparoscopic and open techniques, is essential to control the disease and its complications. Perforation, abdominal abscesses, or adhesions and other abdominal complaints may be observed.
Developmental abnormalities or rare clinical conditions may interfere with the management of the patient with presumed acute appendicitis [1]. These clinical conditions include adenocarcinoma, carcinoid or mucocele of appendix and require careful and close clinical care. Adequate preoperative evaluation and selective usage of imaging techniques such as ultrasonograpy and computed tomography have critical role to recognize such clinical entities [2]. Mucocele of appendix vermiformis is one of these rare clinical conditions, which have potential to result with poor outcomes in some patients due to perforation and pseudomyxoma peritonei [2,3]. Thus, preoperative sufficient surgical evaluation and care should be given for the patients with mucocele appendix in the emergency medicine and surgery.
Here, we have presented and discussed a case with mucocele of appendix vermiformis due to mucinous cystadenoma with carcinoma in situ component.
Case Report
A 36 years old lady presented to the emergency service with abdominal right lower quadrant pain, nausea and loss of appetite. The patient expressed that her abdominal pain continued approximately for one week with increased severity in last two days. On physical examination there was tenderness in the right lower quadrant of the abdomen. Leukocytosis (WBC: 14000 /µL) and elevated C- reactive protein levels (CRP: 5 mg/L) were found in laboratory tests. Her previous medical and surgical history was not significant. The patient was consulted with gynecologist to rule out any gynecological pathology. At the end of the consultation it was reported that there was no emergency gynecological pathology. Than radiological imaging tests were performed. Abdominal radiography was normal.
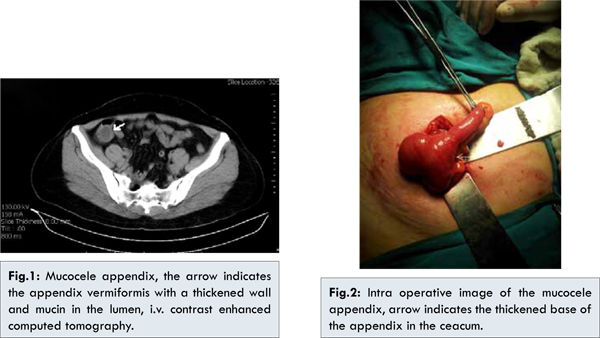
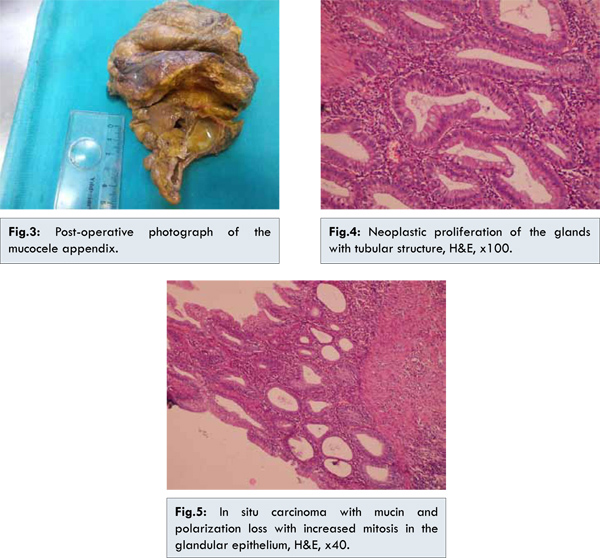
A suspicious lesion was observed on the basis of appendix and caecum in abdominal ultrasonography. Abdominopelvic computed tomography was recommended for further diagnosis. IV contrast enhanced abdominopelvic computed tomography defined a confined lesion in size of 3x2 cm originating from the basis of the appendix and spreading towards the caecum. This lesion was most likely presumed as mucocele of appendix vermiformis [Fig.1]. The patient was hospitalized and laparotomy under general anesthesia was scheduled. A mucocele appendix with a mass (3x2 cm in size) in the base of caecum was observed. For this reason a right hemicolectomy was performed [Fig.2,3]. End to side ileotranversostomy procedure was preferred for anastomosis. Postoperative course was uneventful. Histopathology revealed appendix mucocele due to mucinous cystadenoma with carcinoma in situ component. In details, circumferentially proliferating neoplastic mucinous glands with high grade dysplasia were observed. Proliferating glands were not invading muscularis mucosa, [Fig.4,5]. The patient was consulted with medical oncology and scheduled for routine follow up.
Mucocele of the appendix is a rare cystic lesion of appendix vermiformis which is characterized by an appendix with mucus filled lumen and distended wall [3]. Previously four common subgroups have been defined according to histopathological morphology. These subgroups include retention cysts (18%), mucosal hyperplasia (20%), mucinous cystadenoma (52%) and mucinous cystadenocarcinoma (10%) [4]. Examination of the appendix during surgery cannot differentiate benign or malignant tumors. Thus, careful intra-operative tissue handling is essential to reduce the risk of dissemination of mucin producing epithelium and preoperative imaging should be used vigorously to prevent the complications due to iatrogenic or spontaneous rupture of the mucocele. Pseudomyxoma peritonei is the worst complication, which is characterized by peritoneal dissemination and may be a lethal complication in some patients [5].
Mucocele of the appendix is observed more common in patients older than 50 years and is more frequent among the women [6]. The clinical signs of mucocele of the appendix are unspecific or may be absent. Therefore, detection occurs mostly incidentally by radiologic, ultrasonographic or endoscopic intervention [7]. Clinical signs includes abdominal pain in the right lower quadrant, a palpable mass in slim patients, colic pain in case of obstruction or intussusception, gastrointestinal bleeding and anemia, genitourinary symptoms, or acute abdomen and sepsis in case of a spontaneous rupture of the cyst [8]. CT scanning is the best diagnostic test for preoperative evaluation with high sensitivity rates to detect the rupture of mucocele, peritoneal mucinous carcinomatosis or pseudomyxoma peritonei and wall calcification
[5,9]. In our case, computed tomography has revealed mucocele of appendix vermiformis.
The primary treatment of mucocele appendix is surgical resection. Appendectomy with mesoappendix excision has been advocated to be sufficient for appendiceal masses in the absence of local invasion or cecal involvement. Simple retention cysts usually cause mucocele of appendix which is less than 2 cm in diameter and may be treated with the same fashion. However, hyperplastic epithelium, cystadenoma and cystadenocarcinoma are more likely to be greater than 2 cm in size. For these clinical conditions surgical approach should not be based on diameter alone. Presence of local invasion and cecal involvement should indicate the need for right hemicolectomy [10]. In our case, the base of the appendix was involved with the pathological process. Thus, the patient was treated with right hemicolectomy.
Conclusion
This case underlines the importance of optimal preoperative evaluation and management in the patients with abdominal pain. Surgeons should always beware of and prepared for the rare clinical conditions such as appendicular masses, developmental disorders or mucocele, which are associated with difficult and preventable complications in some patient.
References
- Marudanayagam R, Williams GT, Rees BI. Review of the pathological results of 2,660 appendicectomy specimens. J Gastroenterol 2006;41(8):745-749.
- Gupta S, Sharma R, Attri AK, Kaur R. Mucinous cystadenoma of appendix. Indian J Surg 2008; 70:254-255.
- Gonzalez-Moreno S, Shmookler BM, Sugarbaker PH. Appendiceal mucocele. Contraindication to laparoscopic appendectomy. Surg Endosc 1998;12:1177-1179.
- Higa E, Rosai J, Pizzimbono CA, Wise L. Mucosal hyperplasia, mucinous cystadenoma, and mucinous cystadenocarcinoma of the appendix. A re-evaluation of appendiceal ‘Mucocele’. Cancer. 1973;32(6):1525-1541.
- Gillion JF, Franco D, Chapuis O, Serpeau D, Convard JP, Julles MC, et al. Appendiceal mucoceles, pseudomyxoma peritonei and appendiceal mucinous neoplasms: update on the contribution of imaging to choice of surgical approach. J Chir (Paris) 2009;146(2):150-166.
- Landen S, Bertrand C, Maddern GJ, Herman D, Pourbaix A, de Neve A, et al. Appendiceal mucoceles and pseudomyxoma peritonei. Surg Gynecol Obstet 1992;175:401-404.
- Zanati SA, Martin JA, Baker JP, Streutker CJ, Marcon NE. Colonoscopic diagnosis of mucocele of the appendix. Gastrointest Endosc 2005;62:452-456.
- Ruiz-Tovar J, Teruel DG, Castineiras VM, Dehesa AS, Quindos PL, Molina EM. Mucocele of the appendix. World J Surg. 2007;31:542-548.
- Pickhardt PJ, Levy AD, Rohrmann CA, Kende AI. Primary neoplasms of the appendix: radiologic spectrum of disease with pathologic correlation. RadioGraphics 2003;23:645-662.
- Zagrodnik DF, Rose DM. Mucinous cystadenoma of the appendix: diagnosis, surgical management, and follow-up. Curr Surg 2003, 60:341-343.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
BAYHAN Z, YAYLAK F, DEGER AN, ZENGIN A, ZEYTIN AT, ALGIN MCMucocele of Appendix Vermiformis due to Mucinous Cystadenoma with Carcinoma in Situ Component.JCR 2014;4:169-172 |
|
BAYHAN Z, YAYLAK F, DEGER AN, ZENGIN A, ZEYTIN AT, ALGIN MCMucocele of Appendix Vermiformis due to Mucinous Cystadenoma with Carcinoma in Situ Component.JCR [serial online] 2014[cited 2026 May 27];4:169-172. Available from: http://www.casereports.in/articles/4/1/Mucocele-of-Appendix-Vermiformis-due-to-Mucinous-Cystadenoma-with-Carcinoma-in-Situ-Component.html |

|
|
|
|
|