|
|
|
|
|
Pneumatic Balloon Dilatation of the Trachea: New Hope for Tracheal Stenosis
|
|
|
Sanjeev Mohanty, M. Gopinath
Department of ENT, Head and Neck Surgery, Sri Ramachandra University, Porur, Chennai- 600116, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Sanjeev Mohanty
Email: drsanjeevmohanty@gmail.com
|
|
|
|
|
|
|
|
|
Received:
19-APR-2014 |
Accepted:
22-MAY-2014 |
Published Online:
10-JUN-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Post intubation tracheal stenosis is a clinical problem caused by regional ischemic necrosis of the airway. Its treatment options include tracheal resection with end to end anastomosis, laser resection and stenting. Laser resection followed by balloon dilatation of the soft stenosis is an innovative procedure. It is relatively simple and inexpensive procedure to perform. This case report highlights the importance of this innovative surgical procedure to alleviate the suffering of this elderly diabetic male with chronic renal failure and with a poor cardiac status ‘a high risk surgical patient’. Laser ablation of the stenotic segment followed by balloon dilation was performed under direct visualization. Quality of life following this procedure is also good in relation to post-operative morbidity.
|
|
|
|
|
|
Keywords :
|
Tracheal Stenosis, Respiratory sounds, Constriction, Kidney Failure, Stents.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff4cc905000000b602000001000300 6go6ckt5b5idvals|327 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Tracheal stenosis and the surgical procedure for its optimal management has long been a subject of debate. Incidence of tracheal stenosis has been on the rise due to increased incidence of trauma secondary to road traffic accidents and intubation injuries. Breathlessness on exertion which may be progressive, a brassy cough, recurrent pneumonitis, wheezing, stridor and cyanosis may all be part of the clinical presentation. It frequently has an insidious onset and the symptoms may be mistaken or disregarded for a variety of other disorders. There are multiple causes of benign tracheal stenosis, the most common being trauma. Awareness of the possibility of tracheal stenosis is very important in its early recognition. The management is timely and appropriate surgical intervention. The surgical procedure should be minimally invasive as we are dealing here with the airway and the patients are usually compromised.
Catheter balloon dilatations are being widely performed to dilate areas of narrowing in blood vessels, ureters and the gastrointestinal tract. Balloon dilatation procedures traditionally involve the use of balloon catheters passed over a guide-wire and positioned within the luminal obstruction with the aid of fluoroscopy. While fluoroscopic guidance is necessary when direct visualization is not possible, as is the case with balloon angioplasty, its utility is unclear when an obstruction can be directly visualized, as is the case with balloon dilatation of the trachea. The innovative technique of tracheal dilatation using an oesophageal balloon dilatation is done for the first time to the best of our knowledge.
Case Report
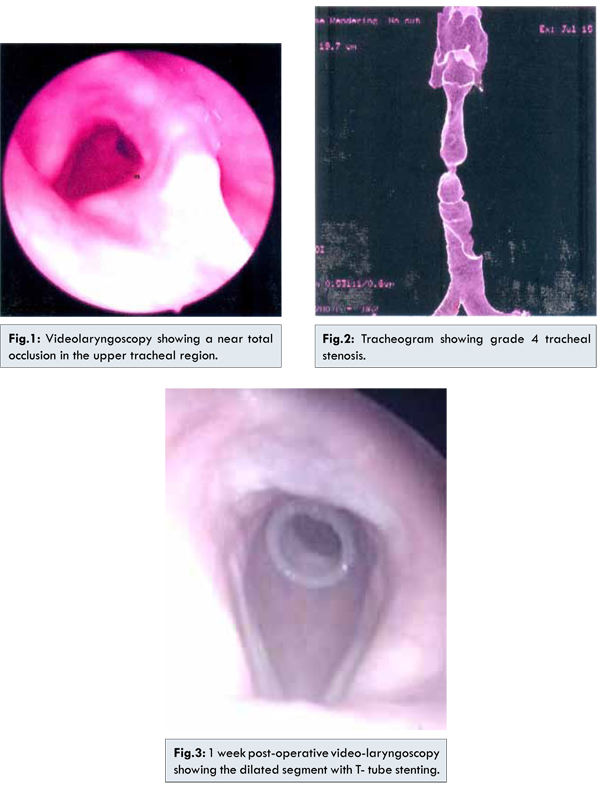
55 year old male was referred by the cardiologist with history of breathing difficulty of 2 weeks duration. Patient had undergone coronary artery bypass graft 10 months back. 6 months post-surgery he developed adult respiratory distress syndrome (ARDS) and was intubated for 3 weeks. His other co-morbid conditions include chronic renal failure and type II diabetes mellitus. He had a poor cardiac status with an ejection fraction of 30%. On clinical examination patient was in biphasic stridor. Video-laryngoscopy done at this time showed stenotic segment in the upper tracheal region except for a small opening in the posterior region [Fig.1]. Vocal cord mobility was normal. To assess the exact site and extent of the stenosis a tracheogram [Fig.2] was done which showed a grade 4 stenotic segment in the upper trachea according to Cotton-Meyer classification. The findings were confirmed with a virtual endoscopy. Our treatment options were either a tracheostomy to relieve the airway obstruction at the cost of his voice or a radical procedure like tracheal resection and end to end anastomosis. Due to his co-morbid conditions he had a high risk and increased morbidity of undergoing a major surgery like tracheal resection and anastomosis. We decided to proceed with the innovative technique of balloon tracheoplasty as it is a conservative procedure as well as curative for the patient. The innovation in this procedure is the use of oesophageal balloon for the dilatation of stenotic segment. Rigid bronchoscope was done and the stenotic segment was visualised. Potassium Titanyl Phosphate (KTP) - 532 laser assisted incision of the stenotic segment was done. Oesophageal balloon was introduced and positioned in the stenotic segment under bronchoscopic guidance. It was inflated with volumetric dosage of air with a pump and the stenotic segment was dilated. This was followed by Montgomery T tube stenting of the stenosed segment [Fig.3]. Post-operatively patient was comfortable and T tube was closed on 2nd post-operative day. Patient was comfortable, phonating well and was discharged on the 2nd post-operative day. Video-laryngoscopy done after 1 week showed the T tube in position and normal vocal cord function. There was no evidence of crusting, edema or granulation at the upper end of the tube. Patient was followed regularly at 3 months interval and decannulated after 1 year.
Apart from trauma, the differential diagnosis of tracheal stenosis can be subdivided into four categories congenital, neoplastic, infectious, and inflammatory [1]. Congenital tracheal stenosis is really quite rare and is often the result of posterior fusion of the tracheal rings, thereby forming complete rings. Other causes of congenital stenosis include vascular rings and other congenital cardiovascular anomalies such as an anomalous subclavian artery [1]. A previous history of endotracheal intubation or tracheostomy should not be taken lightly during the evaluation of a patient with upper airway symptomatology [2,3]. However, if there is no prior history of tracheal trauma, the etiology of the stenosis may be obscure and difficult to determine necessitating a systematic approach to make the diagnosis [4].
The successful management of tracheal stenosis has always been more than a surgical challenge for the otolaryngologists. By far, most cases of benign tracheal stenosis are the result of tracheal trauma, the majority of which are secondary to endotracheal intubation [3]. There are two principal types of strictures that occur after intubation, strictures at the site of the endotracheal tube cuff which is the most common location of post intubation stenosis and those that occur at the site of a tracheostomy stoma. The methods available for treating post intubation stenosis fall into two categories conservative endoscopic and open surgical methods. In our case we decided to go ahead with the innovative technique of balloon tracheoplasty as the treatment option in a patient who had a poor cardiac status and failing kidneys. Oesophageal balloons are primarily used in treating oesophageal strictures, oesophageal variceal bleeding etc. Their use in this part of the airway has not been documented previously. They are cost effective alternative to tracheal balloon dilatation. In contrary to tracheal balloon dilatation where saline or a contrast medium is used, air is used in the oesophageal balloons. Balloon dilatation of the trachea has been first reported by Cohen et al [5]. Balloon dilatation as a primary treatment has not been described in many cases in literature. The combination of laser excision and balloon dilatation was very effective in our case. The use of laser excision and dilatation has been reported earlier with Neodymium Yttrium Aluminium Garnet (Nd-Yag) laser [6,7]. We used the Potassium Titanyl Phosphate (KTP–532) laser in this case. The use of the bronchoscope gave us a good visualization which aided in the laser assisted excision of the stenotic segment [8].
The major advantage of balloon dilatation is lower morbidity and mortality than the open surgical procedures [9,10]. Tracheal lacerations following balloon dilatation have been reported in literature [11]. Caution should be exercised while performing this procedure to prevent complications. Excessive dilatation can lead to airway rupture, mediastinitis, pneumothorax and pneumomediastinum. Bronochoscopic laser assisted surgeries in managing tracheal stenosis is definitely an added advantage in trained hands.
Conclusion
To conclude we emphasize the need for minimally invasive procedures in dealing with high risk patients. Usefulness of oesophageal balloon in tracheal stenosis of recent onset is a worthwhile option as the initial results are encouraging.
References
- Angerpointner TA, Stelter W, Mantel K, Hecker WC. Resection of an intrathoracic stenosis in a child. Prog Pediatr Surg 1987;21:64-71.
- Arola MK, Inberg MV, Puhakka H. Tracheal stenosis after tracheostomy and after orotracheal cuffed intubation. Acta Chir Scand 1981;147:183-192.
- Braidy J, Breton G, Clement L. Effect of corticosteroids on post intubation tracheal stenois. Thorax 1989;44:753-755.
- Bocage JP, Caccavale R, Lewis R, Sisler G, Mackenzie G. Tracheal stenosis. NJ Med 1990; 87:631-634.
- Cohen MD, Weber TR, Rao CC. Balloon dilatation of tracheal and bronchial stenosis. Am J Roentgenol 1984;142:477–478.
- Personne C, Colchen A, Leroy M, Vourc’h G, Toty L. Indications and technique for endoscopic laser resection in bronchology: a critical analysis based upon 2,284 resections. J Thorac Cardiovasc Surg 1986;91:710-715.
- Toty L, Personne C, Colchen A, Vourc’h G. Bronchoscopic management of tracheal lesions using the neodymium yttrium aluminum garnet laser. Thorax 1981;36:175-178.
- Sheski FD, Mathur PN. Long-term Results of Fiberoptic Bronchoscopic Balloon Dilation in the Management of Benign Tracheobronchial Stenosis. Chest 1998;114(3):796-800.
- Hebra A, Powell DD, Smith CD, Othersen HB Jr. Balloon tracheoplasty in children: results of a 15-year experience. J Pediatr Surg 1991;26:957–961.
- Brown SB, Hedlund GL, Glasier CM, Williams KD, Greenwood LH, Gilliland JD. Tracheobronchial stenosis in infants: successful balloon dilation therapy. Radiology 1987;164:475–478.
- Kim YH, Sung DJ, Cho SB, Chung KB, Cha SH, Park HS, et al. Deep tracheal laceration after balloon dilation for benign tracheobronchial stenosis: case reports of two patients. British Journal of Radiology 2006;79:529-535.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Mohanty S, Gopinath M.Pneumatic Balloon Dilatation of the Trachea: New Hope for Tracheal Stenosis.JCR 2014;4:199-202 |
|
Mohanty S, Gopinath M.Pneumatic Balloon Dilatation of the Trachea: New Hope for Tracheal Stenosis.JCR [serial online] 2014[cited 2026 Jul 31];4:199-202. Available from: https://www.casereports.in/articles/4/1/Pneumatic-Balloon-Dilatation-of-the-Trachea.html |

|
|
|
|
|