|
|
|
|
|
A Large Pulmonary Artery Aneurysm in Severe Mitral Stenosis
|
|
|
Mohit Sharma, Siddarth Lukram, Sunil Dixit, Anil Sharma
From the Department of Cardiovascular and Thoracic surgery, S.M.S. Medical College and Group of Hospitals, Jaipur, Rajasthan. |
|
|
|
|
|
Corresponding Author:
|
Dr. Mohit Sharma
Email: aries.mohit@gmail.com
|
|
|
|
|
|
|
|
|
Received:
21-JUL-2014 |
Accepted:
17-SEP-2014 |
Published Online:
20-OCT-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Pulmonary arterial hypertension is commonly present in severe mitral stenosis but a giant pulmonary artery aneurysm is rarely present in severe mitral stenosis. Here, we present a young female 20 years of age admitted to our department for closed mitral valvotomy for severe mitral stenosis. As we opened the thoracic cavity a large size of pulmonary artery aneurysm approximately 10 cm of size was seen, which was not detected pre-operatively by 2-D echocardiography. We operated the case successfully without intervening pulmonary artery aneurysm. Patient recovered well. |
|
|
|
|
|
Keywords :
|
Aneurysm, Hypertension, Lung Diseases, Pulmonary Artery, Echocardiography, Humans, Mitral Valve.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1fff8ff050000003c03000001000100 6go6ckt5b5idvals|380 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Natural history of development of pulmonary arterial aneurysm (PAH) is generally associated with intrinsic wall weakness, increased pulmonary artery (PA) pressure and connective tissue disorder. Increased PA pressure is common and natural pathophysiology in severe mitral stenosis but aneurysmal dilatation is very rare. Here we present a case with giant pulmonary artery aneurysm which was diagnosed intra-operatively. Successful CMV (closed mitral valvotomy) was done and patient recovered well with improvement in symptoms post-operatively. This kind of case needs documentation in medical literature to improve knowledge regarding development of PA aneurysm in severe mitral stenosis cases, especially in Indian
scenario.
Case Report
A 20 years old female patient was admitted to our department with complaints of dyspnea and shortness of breath from 6 months. At the time of presentation she was not having any sign and symptoms of CHF (congestive heart failure) i.e. no pedal edema, no raised jugular venous pressure. On auscultation grade III mid diastolic murmur was present. In chest X-ray left heart border was elevated [Fig.1]. Usually in cases of severe mitral stenosis straightening of the left heart is present in chest X-rays. 2-D Echo revealed that patient was having severe mitral stenosis with mitral valve area of 0.6 cm2, no calcification, no significant tricuspid and aortic disease with normal ejection fraction, PA pressure was right atrial pressure (RAP) + 80. Trans-esophageal echocardiography was also done to confirm any clot or calcification, it was non-calcific mitral stenosis and no clot was present in left atrium and left atrial appendage.

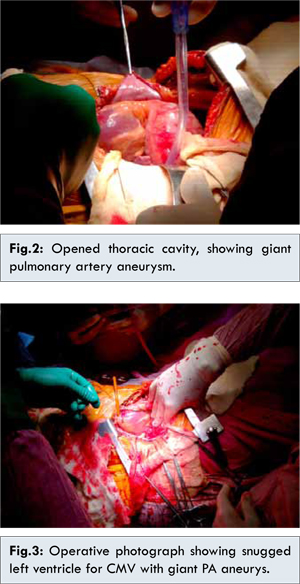
Patient was completely evaluated and planned for closed mitral valvotomy, as the patient was young and having non-calcific mitral stenosis with no LA/LAA (left atrium and left atrial appendage) clot. Patient was taken for surgery; ideal left lateral thoracotomy was done by 5th intercostal space. After opening the thoracic cavity large aneurysmal PA (pulmonary artery) was seen [Fig.2]. Purse string was taken on left ventricular apex and snugged; another purse string was taken on left atrial appendage. After complete hemostasis, index finger was passed through the purse string of left atrial appendage and simultaneously Tubb’s dilator was passed through left ventricular purse string. Mitral valve was opened up to 3.5 cm of Tubb’s dilator. Both purse strings were closed with good hemostasis. After putting chest drain closure was done in layer as in standard thoracotomy. We did successful CMV (closed mitral valvotomy) without intervening PA aneurysm [Fig.3]. Patient recovered well in post-operative period. Patient was discharged on post-operative day 5 with advice of MVR (mitral valve replacement) and PA aneurysm repair afterwards if needed.
In the cases of mitral stenosis increased pulmonary hypertension is common phenomenon. Increased PAH causes shearing stress on vessel wall, if the wall is weak due to associated connective tissue disorder, it can cause aneurysmal dilatation of pulmonary artery. The natural history of giant pulmonary artery aneurysms is not yet defined. In our patient PA pressure was not so high, it was RAP + 80 and there was no connective tissue disorder also. The risk of aneurysm rupture seems very small as in our case as the PA pressure was not so high. Deterling and Clagett reported only eight cases in a review of 1,09,571 necropsies [1]. Giant size pulmonary artery aneurysm (in our patient approx. 10 cm), in the presence of low PA pressures and the absence of left to right congenital or acquired shunts, may not cause high risk in contrast with those with pulmonary hypertension or Eisenmenger’s syndrome [2,3].
Basically true aneurysms involve all the layers of the vessel; it may be associated intimal weakness, and presence of increased hemodynamic shear stresses [4]. Pulmonary arterial aneurysm has been commonly described in patients with left to right shunt with high PA pressure as in patent ductus arteriosus, ventricular septal defect, atrial septal defect, and transposition of the great arteries [2,5]. The management of pulmonary artery aneurysm has largely been surgical. Reported procedures have included graft repair with dacron, pericardium on the main pulmonary artery, and pulmonary arterial aneurysmorrhaphy. In the surgical series of Kuwaki and colleagues [6], aneurysmorrhaphy, without pulmonary valve replacement, was associated with late recurrence of pulmonary arterial dilatation, perhaps because of the persistent hemodynamic stress and defective native pulmonary arterial wall. Management of aneurysm is definitely surgical, at the time of presentation or whenever the complications are there like pulmonary regurgitation.
Conclusion
Our patient was discharged after surgery, which shows simultaneous repair of the aneurysm may not be necessary, it can be repaired in staged surgical approach i.e. during MVR (mitral valve replacement) on cardio pulmonary by-pass.
References
- Deterling RA, Clagett T. Aneurysm of the pulmonary artery: review of the literature and report of a case. Am Heart J. 1947;34:471-499.
- Casselman F, Meyns B, Herygers P, Verougstraete L, Elst FV, Daenen W. Pulmonary artery aneurysm: is surgery always indicated? Acta Cardiol. 1997;52:431-436.
- Daliento L, Somerville J, Presbitero P, Menti L, Brach-Prever S, Rizzoli G, et al. Eisenmenger syndrome: factors relating to deterioration and death. Eur Heart J. 1998;19:1845-1855.
- Keene RJ, Steiner RE, Olsen EJ, Oakley C. Aortic root aneurysm: radiographic and pathologic features. Clin Radiol. 1971;22:330-340.
- Ansari A. Isolated pulmonary valvular regurgitation: current perspectives. Prog Cardiovasc Dis. 1991;33:329-344.
- Kuwaki K, Morishita K, Sato H, Urita R, Abe T. Surgical repair of the pulmonary trunk aneurysm. Eur J Cardiothorac Surg. 2000;18:535-539.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Sharma M, Lukram S, Dixit S, Sharma AA Large Pulmonary Artery Aneurysm in Severe Mitral Stenosis.JCR 2014;4:405-407 |
|
Sharma M, Lukram S, Dixit S, Sharma AA Large Pulmonary Artery Aneurysm in Severe Mitral Stenosis.JCR [serial online] 2014[cited 2026 May 4];4:405-407. Available from: http://www.casereports.in/articles/4/2/A-Large-Pulmonary-Artery-Aneurysm-in-Severe-Mitral-Stenosis.html |

|
|
|
|
|