|
|
|
|
|
A Rare Case of Large Complex Odontoma
|
|
|
Ritesh Kumar Jadav1, Naveen Kumar1, Atul Katarkar2, Jay G. Ray1, Keya Chaudhuri2
1Department of Oral Pathology, Dr R. Ahmed Dental College and Hospital, Kolkata 700014, India. 2Molecular and Human Genetics Division, CSIR-Indian Institute of Chemical Biology, 4Raja S.C. Mullick Road, Kolkata 700032, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Keya Chaudhuri
Email: keya.chaudhuri@gmail.com
|
|
|
|
|
|
|
|
|
Received:
01-OCT-2014 |
Accepted:
12-NOV-2014 |
Published Online:
30-NOV-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Odontomas are hamartomatous developmental malformations of dental tissues. Generally asymptomatic, discovered during the routine radiography, rarely cause expansion of bone followed by facial asymmetry and interfere with teeth eruption. We presents a rare case of complex odontoma in an 11 year old boy which resulted in failure of eruption of permanent 1st and 2nd mandibular left molar. A calcified radiopaque mass was seen in the radiograph and was provisionally diagnosed as odontoma. The tumor was treated by surgical excision under local anesthesia following which the odontoma was enucleated and histologic evaluation was done to confirm the diagnosis. |
|
|
|
|
|
Keywords :
|
Odontoma, Odontogenic tumor, Hamartoma, Tooth eruption, Molar, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff380006000000c202000001001000 6go6ckt5b5idvals|396 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
The term odontoma was first coined by Paul Broca (1866) who defined it as a tumor formed by overgrowth of complete dental tissue [1]. Odontoma is benign developmental anomalies (hamartomas) than true neoplasm or mixed odontogenic tumor hovered with both epithelial and mesenchymal tissues [2]. The exact etiologies behind the odontomas were elusive, may be employed by diverse factors such as local trauma, infection, growth pressure, hereditary and developmental influences [1]. Odontomas are frequently associated with pathologic changes such as impaction, malpositioning, aplasia, malformation, and devitalization of adjacent teeth [3]. Odontomas constitute about 22% of all odontogenic tumors and most common in Caucasian population (65%) and lower in India (5.3%-11.6%) [4,5]. World Health Organization (WHO) classifies odontogenic tumor into complex odontomas (an amorphous conglomeration of dental tissues consisting of enamel, dentin, cementum, pulp and enamel organ) and compound odontomas (many separate, small, tooth-like denticles in a structural and more orderly pattern even rudimentary teeth) [6,7]. Complex odontomas are less common than the compound odontomas in the ratio 1:2.3 [8]. Compound odontomas were common in the incisor-canine region of the maxilla and often occurr in mandibular molar region manifested with bony expansion [3]. There is no gender predilection and odontomas can occur at any age but mean age of occurrence is second decade. Odontomas are treated by surgical excision of the lesion, less possibility of reappearance as it has a limited growth potential but have to be removed at the most primitive stage to avoid cystic change, intervention in eruption and destruction of mandibular bone. We present a rare case of large complex odontoma that resulted in failure of eruption of permanent left mandibular 1st and 2nd molar in a young boy.
Case Report
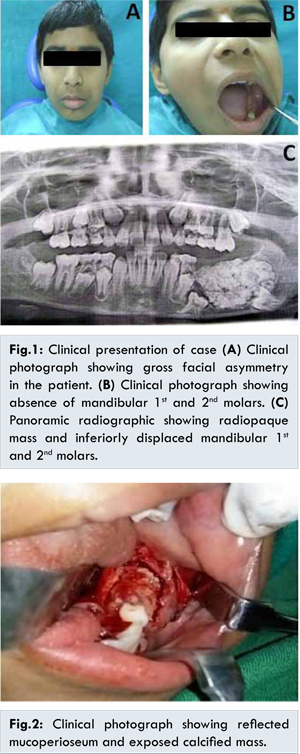
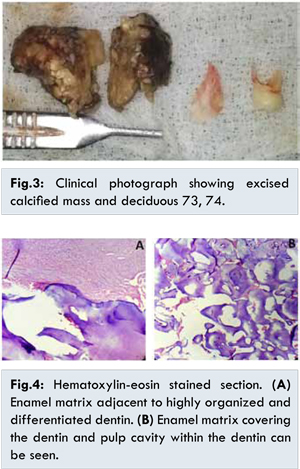
11 year old male patient reported with chief complaint of swelling over the left back tooth region of mandible since 6 months. Asymptomatic 6 months back, he noticed non-tender swelling over left back tooth area which started as small sized swelling and reached present size. Patient was healthy with no dental history and trauma. Extra-oral examination revealed gross facial asymmetry with diffuse smooth swelling in the left mandibular angle [Fig.1A]. Mouth opening was adequate, on palpation the swelling was tender, hard in consistency, noncompressible, and nonreducible. Intraoral examination of the region revealed the apparent absence of the left mandibular 1st and 2nd molar. The buccal and lingual cortical plates were expanded and hard. No signs of inflammation or pus discharge were noticed [Fig.1B]. A panoramic radiograph showed a radiopaque mass (3.5 × 3.3 cm), extending from distal of deciduous 74 to the angle of mandible of same side and overlying the coronal portion of permanent 1st and 2nd molar displaced inferiorly. The left mandibular canal was displaced inferiorly [Fig.1C]. Provisional diagnosis of complex odontoma was made. Intraoral approach was used to access the mass, mucoperiosteal flap reflected, over lying bone was removed and the calcified mass was exposed [Fig.2]. Calcified mass was removed in two parts along with deciduous 73, 74 [Fig.3]. Histopathological examination shows decalcified section enamel matrix appearing as hematoxyphilic fibrillar material due to persistence of prism sheaths while the dentine matrix was eosinophilic and contained tubules [Fig.4A]. The enameloid and dentoid material have disordered arrangement with frequent radial pattern [Fig. 4B]. Histopathological examination confirmed the diagnosis of complex odontoma. The patient was advised a review appointment once in 3 months in order to access the eruption of unerupted tooth and to examine the recurrence of the odontoma. Till date patient was stable and no recurrence was noticed.
It is noteworthy that majority of odontomas in anterior segment of jaw are compound composite type (61%) whereas the majority in posterior segment are complex composite odontoma [9]. Although they are commonly asymptomatic, clinical indicators of odontoma may include retention of deciduous teeth, non-eruption of permanent teeth, pain, expansion of the cortical bone and tooth displacement. Other symptoms include anesthesia in the lower lip and swelling in the affected area. Radiographically, odontoma appear as an irregular radiopacity or denticles surrounded by a radiolucency with or without a bony expansion. There is usually a retained deciduous tooth associated with an unerupted permanent tooth. Unerupted teeth are more commonly associated with compound composite than with complex composite odontoma [10].
In present case report, presence of unerupted tooth with complex composite odontoma was seen. However, etiology of formation of odontoma is still elusive. Odontomas are mostly associated with trauma during primary dentition, as well as with inflammatory and infectious processes, hereditary anomalies (Gardner syndrome, Hermann’s syndrome), odontoblastic hyperactivity and alterations in the genetic components responsible for controlling dental development [11]. Lopez A et al. have concluded in their study that injury occuring early in childhood is more likely to form odontomas. Hitchin suggested odontomas are inherited or due to a genetic mutation or obstruction in postnatal genetic control of tooth development [12,13]. Additionally, large odontomas are associated with local disturbances such as the eruption delay of permanent teeth and the development of cystic lesions as dentigerous cysts. Odontomas are treated by conservative surgical removal and recurrence of complex odontoma is very rare [9,14]. Ameloblastic fibroodontomas and odonto-ameloblastomas show a great resemblance to common odontomas, especially in the radiographic examination. Therefore, it has been suggested that all specimens should be sent to an oral pathologist for microscopic examination [15]. Clinical and radiographic follow-up is cautious where surgical treatment is delayed.
Conclusion
Complex odontomas are rare and should be surgically excised to avoid expansion of cortical plates, craniofacial and tooth developmental problems and pathological fracture of the bone. The periodic clinical and radiographic examination is must in children who present with clinical evidence of delayed or unerupted permanent tooth with or without a history of pervious dental trauma for early diagnosis and better prognosis.
References
- Cohen DM, Bhattacharyya I. Ameloblastic fibroma, ameloblastic fibro-odontoma, and odontoma. Oral and maxillofacial surgery clinics of North America. 2004;16:375-384.
- Neville BW, Damm DD, Allen CM (eds). In: Oral and Maxillofacial Pathology. Philadelphia: WB Saunders; 1995.
- Sheehy EC, Odell EW, Al-Jaddir G. Odontomas in the primary dentition: literature review and case report. Journal of Dentistry for Children (Chicago, Ill) 2003;71:73-76.
- Cildir SK, Sencift K, Olgac V, Sandalli N. Delayed eruption of a mandibular primary cuspid associated with compound odontoma. J Contemp Dent Pract. 2005;6:152-159.
- Yeung KH, Cheung RCT, Tsang MMH. Compound odontoma associated with an unerupted and dilacerated maxillary primary central incisor in a young patient. International Journal of Paediatric Dentistry. 2003;13:208-212.
- Budnick SD. Compound and complex odontomas. Oral Surgery, Oral Medicine, Oral Pathology. 1976;42:501-506.
- Katz RW. An analysis of compound and complex odontomas. ASDC Journal of Dentistry for Children. 1988;56:445-449.
- Tüzüm MS. Orofacial pain associated with an infected complex odontome. Case report. Australian Dental Journal. 1990;35:352-354.
- Neville BW, Damm DD, Allen CM, Bouquot JE. Odontogenic cysts and tumors. Oral and Maxillofacial Pathology. 2002;3:683-687.
- Wood NK, Goaz PW, Lehnert J. Mixed radiolucent-radiopaque lesions associated with teeth. Differential diagnosis of oral and maxillofacial lesions. Singapore: Harcourt Brace & Company Asia Pvt. Ltd. 1998:289-314.
- Ragalli CCs, Ferreria JL, Blasco Fn. Large erupting complex odontoma. International Journal of Oral and Maxillofacial Surgery. 2000;29:373-374.
- Hitchin AD. The aetiology of the calcified composite odontomes. British Dental Journal. 1971;130:475-482.
- Papagerakis P, Peuchmaur M, Hotton D, Ferkdadji L, Delmas P, Sasaki S, et al. Aberrant gene expression in epithelial cells of mixed odontogenic tumors. Journal of Dental Research. 1999;78:20-30.
- López-Areal L, Donat FS, Lozano JG. Compound odontoma erupting in the mouth: 4-year follow-up of a clinical case. Journal of Oral Pathology & Medicine. 1992;21:285-288.
- Shafer WG, Hine MK, Levy BM, Tomich CE. A Textbook of Oral Pathology: Saunders Philadelphia; 1983.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Jadav RK, Kumar N, Katarkar A, Ray JG, Chaudhuri KA Rare Case of Large Complex Odontoma.JCR 2014;4:467-470 |
|
Jadav RK, Kumar N, Katarkar A, Ray JG, Chaudhuri KA Rare Case of Large Complex Odontoma.JCR [serial online] 2014[cited 2026 Mar 20];4:467-470. Available from: http://www.casereports.in/articles/4/2/A-Rare-Case-of-Large-Complex-Odontoma.html |

|
|
|
|
|