|
|
|
|
|
Glomus Tumor of Face
|
|
|
progesterone basse progesterone naturelle click here
From the Departments of Surgery and Pathology, Katihar Medical College, Katihar-854105, Bihar, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Tushar Singh
Email: tusharsingh020785@gmail.com
|
|
|
|
|
|
|
|
|
Received:
05-AUG-2014 |
Accepted:
13-OCT-2014 |
Published Online:
15-NOV-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Glomus tumor is a neoplastic proliferation of glomus body, which is a thermoregulatory neuromyoarterial unit seen predominantly in the subungual regions. These tumors are found mainly in the digits. Extra digital location is uncommon and involvement of face is rare. However, possibility of glomus tumor in a subcutaneous nodule of face should be considered particularly if it shows typical triad of intense paroxysmal pain, exquisite tenderness and sensitivity to cold. Though, the typical findings may be absent. Diagnosis depends upon high index of suspicion. Histopathological examination of the lesion confirms the diagnosis. Here, we present a case of 29 years old male who presented with a small painless subcutaneous nodule on the face.
|
|
|
|
|
|
Keywords :
|
Glomus Tumor, Neoplasms, Face, Pain, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff1c00060000004503000001000a00 6go6ckt5b5idvals|389 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Glomus tumor arises from glomus body, a neuromyoarterial unit located in stratum reticularis of dermis [1]. It accounts for 1-2% of soft tissue tumor and is seen predominantly in subungual region of digits [2]. Extra digital location for the tumor has been described, but face is considered to be rare site. In a study, out of 56 cases of extra digital glomus tumor seen at Mayo clinic over a period of 20 years (1985-2005), only one case was reported in cheek [3]. Clinical presentation includes triad of intense paroxysmal pain, exquisite tenderness and sensitivity to cold [4]. These features may or may not be present in cases of glomus tumor of face and patient may present with asymptomatic subcutaneous nodule or chronic facial pain. Biopsy is needed for diagnosis and is therapeutic as well in many cases.
Case Report
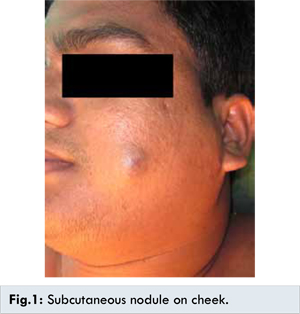
29 years old male presented with a painless swelling over left cheek since 4 months. Examination revealed a non-tender, well defined, smooth, soft and bluish swelling of about 2x2 cm on left side of face [Fig.1]. There was no clinically palpable node in the neck. Examination of oral cavity was within normal limits. Fine needle aspiration cytology (FNAC) of the lesion was obtained. It was reported to have moderately cellular, scattered and dissociated cluster of cells with mild anisonucleosis, bland nuclear chromatin and scanty cytoplasm along with plasmacytoid cells showing bluish cytoplasm and cytoplasmic vacuoles. Lymphocytes and few macrophages were seen in the background. Features were considered to be suggestive of benign adnexal tumor.
Patient was scheduled for surgery. The swelling was excised completely through a skin-crease incision and sent for histopathological examination. On HPE it was found to have branching vessels lined by endothelial cells and surrounded by sheets of small round cells with round bland nuclei and eosinophilic cytoplasm [Fig.2]. There were also nests and aggregates of these cells in stroma. Occasional chronic inflammatory cells were present in stroma. Based on these findings diagnosis of glomus tumor was made.
Discussion
Glomus tumor is a neoplasm of glomus body, first described by Wood in 1812. Masson in 1924 provided the first clinical description for this condition [4]. The tumor develops from glomus body, which is a specialized arterio-venous fistula situated in stratum reticularis of dermis. The arterial end of the body is known as Sucquet-Hoyer canal and is lined by modified smooth muscle cell called glomus cell, derived from Zimmerman pericyte. Its contraction leads to heat preservation and dilatation to heat loss and thus plays an important role in thermoregulation [1,5,6].
According to WHO classification, glomus tumor can be divided into three subtypes depending upon the predominance of different histological component. A tumor having predominant vascular component is known as glomangioma, while that with predominant muscular component as glomangiomyoma and predominant cellular component as solid. Other variants include (i) glomangiomyomatosis - A benign and diffuse form (ii) symplastic glomus tumor - Tumor with marked nuclear atypia, considered a degenerative phenomena in absence of other malignant feature and (iii) glomangiosarcoma - the malignant variant, accounts for 1% of all glomus tumor [7]. Glomus body is predominantly located in palms, digits and soles and so the glomus tumors are usually seen in limbs particularly in subungual regions of digits [5]. Extra digital location of glomus tumor has been described. It includes face, colon, stomach, lung, bone, nervous system and fallopian tube [3]. Extra-digital glomus tumors are more common in men and male outnumber the female by a ratio is 4:1 [3]. Usually these tumors do not exceed the size of 1x1 cm, but large glomangiomas mimicking venous malformation have been reported. MRI is considered to be the most sensitive investigation for glomus tumor in extremity.
Excisional biopsy usually settles the diagnosis. The characteristic appearance of glomus cells and nesting pattern referred to as zellbalen is usually sufficient to establish the diagnosis on routine microscopy. Though in cases, where these features are not evident, immunohistochemistry may help to reach the conclusion. According to Rallis et al. IHC profile that suggests the diagnosis of glomus tumor is immunopositivity with smooth muscle actin, muscle spindle actin and vimentin and negative immune reactivity with S-100 and epithelial marker [8].
Treatment is adequate surgical excision; though, recurrence can be seen in 12-33% of cases. Recurrence occurring within days to weeks indicates inadequate surgical excision while 2-3 years after may be because of multiple tumor [9].
In our case, patient presented with an asymptomatic subcutaneous nodule on face, which on excision and biopsy was proved to be glomus tumor. Since complete excision was already performed at initial surgery, no further intervention was required. Post-operative recovery was excellent and patient didn’t reveal any sign of recurrence in follow up period of six months.
Conclusion
Glomus tumor of face is a rare condition and only presentation may be an asymptomatic subcutaneous nodule. Complete surgical is usually curative & overall prognosis is good.
References
- Fletcher C. Tumours of blood vessels and lymphatics. In: Diagnostic Histopathology of Tumors. Churchill Livingstone, Edinburgh, UK; 2000: pp.75-76.
- Enzinger SW, Weiss FM. Soft Tissue Tumors. Mosby, St.Louis, Mo, USA, 3rd edition; 1995.
- Schiefer TK, Parker WL, Anakwenze OA, Amadio PC, Inwards CY, Spinner RJ. Extradigital glomus tumors: a 20-year experience. Mayo Clinic Proceedings. 2006;81:1337-1344.
- Tomak Y, Akcay I, Debak N, Eroglu L. Subungual glomus tumors of the hand: diagnosis and treatment of 14 cases . Scand J Plastic Reconstruction Surgery Hand Surgery. 2003;37:121.
- TB Fitzpatrick, RA Johnson, K Wolf, MK Polano D. Suurmond. Color Atlas and Synopsis of Clinical Dermatology, McGraw-Hill, 3rd edition;1997.
- Venkatachalam MA, Greally JG. Fine structure of glomus tumor: similarity of glomus cells to smooth muscle Cancer. 1969;23(5):1176-1184.
- Fletcher DC, Unni KK, Mertens F (eds). Glomus tumors, in World Health Organization Classification of Tumors. Pathology and Genetics of Tumors of Soft Tissue and Bone. Lyon, IARC Press; 2002: pp. 137.
- Rallis G, Komis C, Mahera H. Glomus tumor: A rare location in the upper lip. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:327.
- Saglam Y, Basak K, Köse HI, Kiliçkap Y, Karadayi N. Glomus Tumor of Nasal Cavity. Journal of Case Reports. 2014;4(2):375-378.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Muslim S, Singh T, Kumar R, Arif M.Glomus Tumor of Face.JCR 2014;4:443-445 |
|
Muslim S, Singh T, Kumar R, Arif M.Glomus Tumor of Face.JCR [serial online] 2014[cited 2026 May 26];4:443-445. Available from: http://www.casereports.in/articles/4/2/Glomus-Tumor-of-Face.html |

|
|
|
|
|