|
|
|
|
|
Glomus Tumor of Nasal Cavity
|
|
|
augmentin sciroppo augmentin mha.dk
1Department of Pathology, Dr. Lütfi Kirdar Kartal Education and Research Hospital, Istanbul, Turkey; 2Clinic of Otorhinolaryngology, Remedy Hospital, Pendik, Istanbul, Turkey. |
|
|
|
|
|
Corresponding Author:
|
Dr. Yasin Saglam
Email: myasinsaglam97@hotmail.com
|
|
|
|
|
|
|
|
|
Received:
20-JUN-2014 |
Accepted:
05-SEP-2014 |
Published Online:
05-OCT-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Glomus tumor is a vascular tumor that originates from glomus body. It is typically seen in young adults and localized in distal extremities and nail beds. It often presents with stuffiness, rhinorrhea and pain. Glomus tumor is rare in the head and neck region. A 79 year-old-male who presented with stuffiness and ear congestion, was found to have a mass located in the posterior of the nasal cavity on rhinoscopic examination. Macroscopically, the excisional biopsy of the mass had an irregular surface and hyperemia. Pathology of the biopsy showed that the lesion consisted vascular structures, which were surrounded by solid epithelioid, acidophilic and smooth muscle actin positive cells. The case was diagnosed as nasal glomus tumor. |
|
|
|
|
|
Keywords :
|
Glomus Tumor, Nasal Cavity, Paranasal Sinuses, Pain, Arteriovenous Anastomosis, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff3cf805000000fa02000001000a00 6go6ckt5b5idvals|372 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Glomus tumor is a vascular benign tumor that develops from the modified smooth muscle in glomus body [1]. It originates from the proliferation of arteriovenous capillary anastomosis [2]. Glomangioma, solid glomus tumor and glomangiomyoma are the histologic variants of classic glomus tumor. The distinction between these three variants is made according to the composition of glomus cells, vascular structures and smooth muscle cells [3]. Glomus tumor is typically seen in digital areas and the nail bed [4]. We present here a rare case of nasal glomus tumor.
Case Report
A 79 year old male presented with increased stuffiness and ear congestion on the right side for two months. Examination revealed, a 2.5 cm mass having rough surface with a hyperemic appearance and clinically regular/smooth margins. Tympanic membrane was dull, nasal septum was deviated to the right on the posterior and there was a hyperemic mass that has blocked the passage in the nasal cavity. Family history, laboratory findings and past medical history were had no important feature.
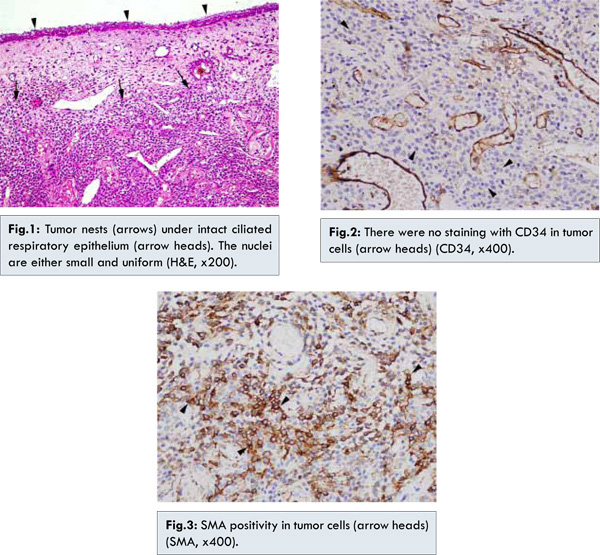
Gross material was grey tan colored and 2.5x1.2x0.5 cm in diameter. The specimen was fixed at 10% buffered-formalin, embedded in paraffin, 5µ sections were cut, stained with haematoxylin eosin, CD34 (clone QBEnd/10, 1/100 dilution; Biocare, CA, USA) and smooth muscle actin (SMA) (clone 1A4, 1/300 dilution; Biocare, CA, USA). Microscopically, pseudostratified ciliated columnar epithelial with goblet cells on the surface, vascular structures lined with endothelial cells and solid proliferating epitheloid cells with round-oval nuclei and acidophilic cytoplasm were observed [Fig.1]. Since there were no high nuclear grade or atypical mitosis and the mass was located superficially, it was considered as benign. Hemangioma was included in the differential diagnosis. Vascular endothelial cells were immunoreactive with CD34 [Fig.2] while the solid epitheloid cells were not. Immunoreactivity for SMA [Fig.3] around the vascular structures ruled out hemangioma and the case was considered as glomus tumor. Since the primary treatment of glomus tumor is surgical excision, no advanced treatment was planned.
Glomus body is a specialized arteriovenous anastomosis in the dermis, which plays a role in thermoregulation [5]. Glomangioma is a benign soft tissue tumor locating in distal extremities, nail bed and subcutaneous tissue [6]. Glomangiomas account for 0.4% of nasal cavity tumors, paranasal sinus tumors and epithelial tumors of nasopharynx [7]. Patients often show nonspecific symptoms. There may be one or more of stuffiness, rhinorrhea and nasal facial pain. In a study, man and woman ratio was found as 1:2, the age range as 28-49 and the mean age as 55 [1]. The nasal glomus tumor may also be seen in young ages [8]. Macroscopically glomus tumors are often seen as blue-red, round, rigid nodules and usually less than 1 cm in diameter [9].
Microscopically they are well circumscribed solid neoplasms and composed of round and polygonal glomus cell clusters. There are cells with large nuclei and narrow eosinophilic cytoplasm [4]. The vascular structures were surrounded by epithelioid cells [9]. Invasion may be seen in glomus tumor [10]. Stromal background may contain patchy mucoid degeneration, hyalinization and hemosiderin probably due to old traumas [5]. The smooth muscle cells that forms glomus tumor are immunoreactive for SMA and thus, glomus tumor is distinguished from hemangiopericytoma [11]. The local recurrence rate of glomus tumor is 10% [3]. It may be more than 30% in cases of incomplete excision [1]. Glomangiosarcoma, the malignant variant of glomus tumor, has a potential of invasion and metastasis and it can easily be distinguished from benign glomus tumors histopathologically [12]. Glomangiosarcoma in nasal cavity has not been reported so far [1]. Treatment of glomus tumor is total excision of the mass and if so, the prognosis is excellent [2].
In our case, glomus tumor was located in the nasal cavity. The patient presented with nasal and ear obstruction symptoms. The surgical excision material was 2.5 cm in diameter, irregular, gray-tan colored and hyperemic. These features are apart from the characteristics of glomus tumor, since tumors has been reported as round and less than 1 cm in diameter. Our patient was 79 years old, in the expected age range. Microscopically, our case was suitable for overall profile and this provided us diagnostic clues despite the atypical localization of the tumor. The probability of malignancy was also considered, but absence of atypical mitotic figures, invasion or any evidence of metastasis, allowed us to exclude malignancy. Tumor invasion was not detected by examining preparations. This enabled us to rule out invasive glomus tumor, which is also benign and should be in the differential diagnosis. There were no hyalinization, hemosiderin or mucoid degeneration in the stroma. Immunoreactivity for SMA, vascular endothelial immunoreactivity for CD34 and no immunoreactivity in the surrounding epitheloid cells are suitable for classical glomus tumor characteristics. Hemangiopericytoma, the most important tumor in differential diagnosis, was excluded since the absence of the characteristic appearance that will create a clear distinction and the immunoreactivity for SMA which showed us the lesion contained smooth muscle cells. Increased ratio of local recurrence of glomus tumor from 10% to 30% in incomplete excision, showed that complete excision is certainly required. Advanced treatment was not needed since the mass was totally excised two years ago and thus, the prognosis will be excellent. The patient has not presented with any complaint about the lesion location during recovery.
References
- McKenna J, Kerr PD. Glomangioma of the nasal cavity. Journal Otolaryngology Head and Neck Surgery. 2008;37(1):E5-7.
- Arens C, Dreyer T, Eistert B, Glanz H. Glomangioma of the nasal cavity. Case report and literature review. Journal for Oto-Rhino-Laryngology and its Related Specialties. 1997;59(3):179-181.
- Constantinidis J, Kiefer A, Reitnauer K, Iro H. Glomangioma of the nasal cavity and paranasal sinuses. Rhinology. 2000;38(3):136-139.
- Shek TW, Hui Y. Glomangiomyoma of the nasal cavity. American Journal of Otolaryngology. 2001;22(4):282-285.
- Ahmed A, Sheehan AL, Dugar J. Intranasal glomangioma. Rhinology. 2003;41(1):58-60.
- Duclos JY, Duffas O, Deminière C, Darrouzet V, Stoll D. [Glomangioma or “glomus tumor” of the nasal cavity: apropos of a new case and review of the literature]. Revue de Laryngologie Otologie Rhinologie. 2001;122(2):119-123.
- Fu YS, Perzin KH. Non-epithelial tumors of the nasal cavity, paranasal sinuses, and nasopharynx: A clinicopathologic study. I. General features and vascular tumors. Cancer. 1974;33(5):1275-1288.
- Chu PG, Chang KL, Wu AY, Weiss LM. Nasal glomus tumors: report of two cases with emphasis on immunohistochemical features and differential diagnosis. Human Pathology. 1999;30(10):1259-1261.
- Cullen RD, Hanna EY. Intranasal glomangioma. American Journal of Otolaryngology. 2000;21(6):402-404.
- Gaut AW, Jay AP, Robinson RA, Goh JP, Graham SM. Invasive glomus tumor of the nasal cavity. American Journal of Otolaryngology. 2005;26(3):207-209.
- Bertalot G, Falchetti M, Parafioriti A. Glomus tumour: The immunohistochemical characteristics of twenty-three cases. Pathologica. 1994;86(5):509-512.
- Alarcos LA, Matesanz SA, Alarcos TE, Ovelar AY. A glomus tumor of the nasal fossa and ethmoid sinus. Acta Otorrinolaringológica Española. 1992;43(4):291-295.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Saglam Y, Basak K, Köse HI, Kiliçkap Y, Karadayi NGlomus Tumor of Nasal Cavity.JCR 2014;4:375-378 |
|
Saglam Y, Basak K, Köse HI, Kiliçkap Y, Karadayi NGlomus Tumor of Nasal Cavity.JCR [serial online] 2014[cited 2026 May 13];4:375-378. Available from: http://www.casereports.in/articles/4/2/Glomus-Tumor-of-Nasal-Cavity.html |

|
|
|
|
|