|
|
|
|
|
Left sided Acute Appendicitis in a Patient with Midgut Malrotation
|
|
|
prednisolon 5 mg prednisolon og alkohol read here partial birth abortions buy abortion pill
From the Department of Surgery, Bhakti Vedanta Hospital & Research Institute, Srishti Complex, Mira Road East, Thane, Maharashtra – 401017, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. BC Shah
Email: vaishnavasevadasa@gmail.com
|
|
|
|
|
|
|
|
|
Received:
23-JUN-2014 |
Accepted:
16-JUL-2014 |
Published Online:
05-AUG-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Appendicitis is typically established when a patient presents with peri-umbilical abdominal pain associated with nausea or vomiting and subsequent radiation of the pain to the right iliac fossa. Rarely, left sided appendicitis has been reported in the literature and when it occurs invariably it is associated with a congenital anomaly of the abdomen either situs inversus or intestinal malrotation. We present here, a case of acute appendicitis in a patient with intestinal malrotation. |
|
|
|
|
|
Keywords :
|
Appendicitis, Abdominal pain, Nausea, Vomiting, Situs Inversus.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff9ce8050000000e03000001000200 6go6ckt5b5idvals|348 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Intestinal malrotation is a rare congenital entity comprising non-rotation and incomplete rotation of the primitive intestinal tube around the axis of the superior mesenteric artery [1]. Usually the diagnosis is mostly incidental, based on investigations carried out for unrelated symptoms, especially in adults [2]. We present here, such a case of malrotation identified due to acute abdominal pain on the left lower quadrant of the abdomen and diagnosed as acute appendicitis.
Case Report
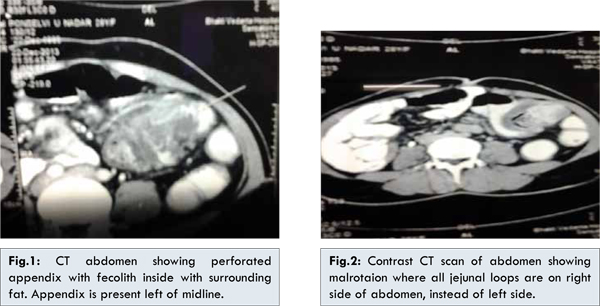
A 30 year old female presented with complaints of sudden onset of severe generalized abdominal pain associated with vomiting since two hours. There was no significant past history of any medical or surgical illness. Physical examination findings included generalized tenderness over the abdomen associated with guarding in the region of left iliac fossa. All the biochemical and hematological investigations were performed and the only significant laboratory finding was a raised total leukocyte count. Ultrasonography of the abdomen revealed a fluid collection in the left iliac fossa with dilatation of small bowel loops. Contrast enhanced computed tomography (CECT) of the abdomen and pelvis [Fig.1,2] showed dilated small bowel loops with most of the jejunal loops lying on the right side of the abdomen; ascending colon and appendix were observed to lie on the left side to the midline; appendix was found to be swollen and severely inflamed with a large faecolith inside. Additionally, a lump with abscess collection around the appendix was observed. Due to the concomitant presence of appendicular lump and intestinal malrotation along with the patient’s preference to undergo laparoscopic procedure than open laparotomy, the patient was managed conservatively with appropriate antibiotics and analgesics. Laparoscopic appendectomy was carried out after four weeks of diagnosis and appendix was found lying left of the midline with type 1A midgut malrotation. The post-operative period was uneventful and the patient was discharged without any complications.
We had presented here a rare case of congenital malrotation of the intestine presenting with acute appendicitis in adulthood. Appendicitis is the most common abdominal emergency surgical condition reported to occur in around 2-3 per 1000 individuals without predilection to any gender. The typical presentation of appendicitis include peri-umbilical onset of abdominal pain associated with nausea gradually shifting to the McBurney’s point in the right iliac fossa. Although various scoring systems exist such as modified Alvarado score, Ohmann score and Eskelinen score, none of these predict appendicitis in all the patients [3]. The diagnosis is often confirmed by abdominal ultrasound and computed tomography. The only significant laboratory finding will be leukocytosis in 90% of the patients with appendicitis. But, when a patient presents with left sided lower abdominal pain, the first suspicion will be of diverticulitis. Unless imaging is done, it is clinically impossible to diagnose appendicitis (which is a very rare condition with this presentation) when there is pain arising from the left lower abdominal quadrant. Even in the present case, the diagnosis was established following CECT. Left sided appendicitis usually occurs in association with other congenital anomalies and rarely the right sided appendix may be lengthier to extend to the left side [4]. A short review of 95 cases of left-sided appendicitis published between 1893 to 2010 revealed that 66 patients had situs inversus totalis, 23 had midgut malrotation [5]. Intestinal malrotation occurs due to errors in the rotation of the midgut around the superior mesenteric artery during the 5th-10th week of fetal development and occur in one out of every 500 newborns (0.2%) ranging between 0.03-0.5% [6]. Approximately 2/3rd of the patients with intestinal malrotation present during the neonatal period and 1/5th present during infancy. Presentation of intestinal malrotation in adults is mostly asymptomatic. Several classifications exist regarding the types of intestinal malrotation such as Balthazar and Stringer. Our patient had type 1A malrotation according to Stringer classification which was the non-rotation of duodenum and colon. In this form, the duodenum and large bowel stop rotating after 90°, so that the proximal small bowel, including the duodeno-jejunal junction, lies on the right and cecum lies on the left. The patient was asymptomatic during his life and was not diagnosed until the onset of acute pain. The location of her pain prevented correct clinical diagnosis, resulting in rupture and advanced disease.
Conclusion
Atypical presentation of the acute appendicitis in a patient with intestinal malrotation may lead to delay in diagnosisand subsequently the appropriate therapeutic management. Left-sided acute appendicitis should be considered in the differential diagnosis of patients with localized pain in the left lower quadrant and computed tomography shall be performed to confirm the diagnosis.
References
- Pickhardt PJ, Bhalla S. Intestinal malrotation in adolescents and adults: spectrum of clinical and imaging features. Am J Roentgenol 2002;179:1429-1435.
- Emanuwa OF, Ayantunde AA, Davies TW. Midgutmalrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J Emerg Surg 2011;6:22.
- Tawk CM, Zgheib RR, Mehanna S. Unusual case of acute appendicitis with left upper quadrant abdominal pain. International Journal of Surgery Case Reports. 2012;3:399-401.
- Hou SK, Chern CH, How CK, Kao WF, Chen JD, Wang LM, et al. Diagnosis of appendicitis with left lower quadrant pain. J Chin Med Assoc. 2005;68:599-603.
- Akbulut S, Ulku A, Senol A, Tas M, Yagmur Y. Left-sided appendicitis: Review of 95 published cases and a case report. World J Gastroenterol 2010;28:5598-5602.
- Badea R, Al Hajjar N, Andreica V, Procopet B, Caraiani C, Tamas-Szora A. Appendicitis associated with intestinal malrotation: imaging diagnosis features. Case report. Medical Ultrasonography 2012;14:164-167.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Shah BC, Degloorkar S, Rao ALeft sided Acute Appendicitis in a Patient with Midgut Malrotation.JCR 2014;4:283-285 |
|
Shah BC, Degloorkar S, Rao ALeft sided Acute Appendicitis in a Patient with Midgut Malrotation.JCR [serial online] 2014[cited 2026 Apr 9];4:283-285. Available from: http://www.casereports.in/articles/4/2/Left-sided-Acute-Appendicitis-in-a-Patient-with-Midgut-Malrotation.html |

|
|
|
|
|