|
|
|
|
|
Metastatic Breast Carcinoma Associated with Numb Chin Syndrome
|
|
|
benadryl and pregnancy nausea benadryl and pregnancy
From the Departments of Medicine and Radiology1, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences (NEIGRIHMS), Mawdiangdiang, Shillong, Meghalaya-793018, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Bhupen Barman
Email: drbhupenb@gmail.com
|
|
|
|
|
|
|
|
|
Received:
03-NOV-2014 |
Accepted:
10-DEC-2014 |
Published Online:
30-DEC-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Numb chin syndrome (NCS) is the presence of hypoesthesia or paraesthesia of the lip and chin in the region of the distribution of inferior alveolar or mental nerve, often caused by metastatic malignancy. We present a 52 year old female known case of rheumatoid arthritis with past history of modified radical mastectomy for right breast carcinoma presenting with paraesthesia and intermittent pain in left lower facial area. CECT abdomen showed liver metastasis and MRI of the head and neck region showed metastatic lesion in the mandible along with vertebral metastasis. Diagnosis of numb chin syndrome was made and patient was put on symptomatic management. Though rare, the NCS may be first symptom in the presentation of underlying malignancy. The treating physician must be aware that the seemingly trivial symptom of lower facial numbness may signal serious illness and early diagnosis do have significant improvement of the treatment course and prognosis. |
|
|
|
|
|
Keywords :
|
Breast Neoplasms, Carcinoma, Chip, Hypesthesia, Lip, Mastectomy, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff7000060000006903000001000100 6go6ckt5b5idvals|410 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Numb chin syndrome (NCS), also known as “mental neuropathy” is a sensory neuropathy characterised by oro-facial paraesthesia typically localised to the chin and lower lip involving the distribution of inferior alveolar or mental nerve and its branches [1]. This rare neurological condition, often underappreciated, has been documented as the initial symptom of a malignant disease in various case reports or small studies. This is a pure sensory neuropathy as the inferior alveolar nerve has no motor fibres. Symptoms of this syndrome are usually caused by malignant cell infiltration of the inferior alveolar nerve sheath or by direct compression by a local tumor or metastatic deposits involving mandible. This can be a very ominous sign as it may not only indicate metastasis from distant tumour but may be the first manifestation of systemic malignancy [2]. Here we report a case of numb chin syndrome as a presenting manifestation of metastatic breast carcinoma.
Case Report
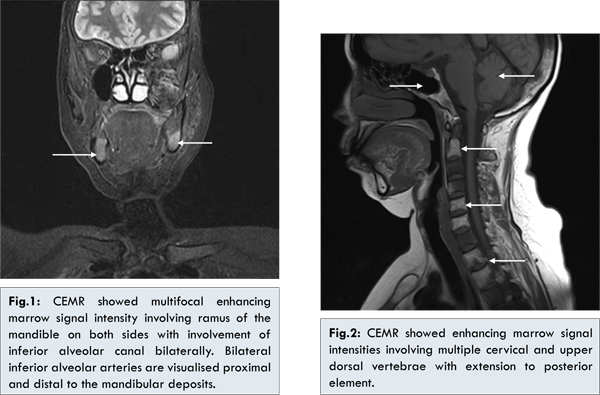
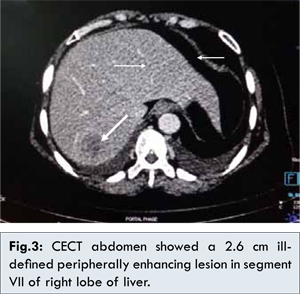
A 52 year old female presented with progressive hypoesthesia and paraesthesia of the chin and the left angle of the mouth, associated with intermittent pain and tingling sensation of about 2 weeks’ duration prior to the hospital admission. She was a known case of seropositive rheumatoid arthritis and was on disease modifying anti-rheumatic drugs for a long time (methotrexate and hydroxy-chloroquine with intermittent oral steroid). She was a patient of carcinoma breast (infiltrating duct carcinoma of the right breast) without metastasis and had undergone modified radical mastectomy of the right breast in March, 2013 (Modified Bloom Richardson grading: grade II). Postoperatively, the patient was asymptomatic for her malignancy till one month prior to her present hospitalization, when she started having pain and tingling sensation over the lower part of her face. On examination there was no sign of local dental pathology. However, there was absence of pain and touch sensation over the chin and left angle of the mouth. There were no other neurological deficits and other systems were clinically normal. The chest x-ray and routine blood reports were within normal limits. Her CECT abdomen showed focal hepatic lesion in segment VII of right lobe of liver with multifocal bony sclerosis involving dorso-lumbar vertebrae, sacrum, iliac bone and right 7th rib suggestive of disseminated metastasis. MRI head and neck also showed multifocal enhancing marrow signal intensities involving vertebrae (including posterior element), mandible and calvarium, suggestive of bone metastasis. Patient was put on palliative chemotherapy and symptomatic management [Fig.1-3].
Neuropathy of the inferior alveolar nerve or mental nerve is a rare neurologic disorder, most often associated with malignancy. It was first described in 1830 by Charles Bell in a lady with breast cancer presenting with numbness of chin due to compression of inferior alveolar nerve [3]. Later on, in 1963, Calvery et al. coined the term numb chin syndrome (NCS) for this presentation [4]. Various aetiologies of NCS have been reported, however malignancy is one of the most common causes of NCS and can represent widespread metastatic disease and often being its first clinical presentation [5]. The most common organs of origin due to metastasis are breast, lung, stomach, thyroid, prostate, kidney and lymphoproliferative neoplasms. Non-malignant causes include local trauma, infections, tumour and cyst, immune mediated systemic diseases like Takayasu arteritis, multiple sclerosis, sickle cell disease, syphilis, sarcoidosis and systemic vasculitis [5].
There are several pathogenic mechanisms for NCS [6]: (i) compression of the mental or inferior alveolar nerve by metastasis to mandible, (ii) metastasis to skull bone, and (iii) leptomeningeal spread. The diagnosis of this rare syndrome is clinical, although, various radiographic studies are helpful to confirm the diagnosis. But it is the clinicians’ ability to recognise the classical symptoms of chin or lip numbness that may point to a serious underlying illness.
Imaging studies that are helpful in the diagnosis of NCS are panoramic jaw radiography, CT scan, MRI and nuclear bone scintigraphy of the head and neck region. Radiographic findings includes osteoblastic or osteolytic lesion in the mandible or in the region of mental foramen along with underlying dental pathology. Imaging of brain and skull bones can also be useful as it may reveal proximal lesions affecting the mandibular division of trigeminal nerve. Lumber puncture with CSF analysis may also be necessary to exclude carcinomatous meningitis or leptomeningeal metastasis if imaging studies fail to reveal an anatomic lesion.
Treatment of NCS is mainly based on underlying cause and management of symptoms. Prognosis of patients with NCS due to malignancy is very poor with median survival following diagnosis may be approximately 5 months in case of mandibular metastasis and 12 months in case of leptomeningeal sedding [6].
Conclusion
Though rare, NCS should be considered on differential diagnosis when patient presents with unilateral numbness of lip or chin. If local dental diseases are excluded, one should consider for the possibility of metastatic cancer, usually breast cancer or lymphoproliferative neoplasms. Radiological evaluation with CT or MRI is helpful in the diagnosis.
References
- Zaheer F, Hussain K, Rao J. Unusual presentation of ‘numb chin syndrome’ as the manifestation of metastatic adenocarcinoma of the lung. International Journal of Surgery Case Reports. 2013;4:1097-1099.
- Baskaran RK, Krishnamoorthy, Smith M. Numb Chin Syndrome-a reflection of systemic malignancy. World J Surg Oncol. 2006,4:52.
- Furukawa T. Charles Bell’s description of numb chin syndrome. Neurology. 1988; 38:331.
- Calverley JR, Monhac AM. Syndrome of numb chin. Arch Intern Med. 1963;112:819-821.
- Marinella MA. Numb Chin Syndrome: A Subtle Clue to Possible Serious Illness. Hospital physician; January 2000:54-56.
- Lossos A, Siegal T. Numb chin syndrome in cancer patients: etiology, response to treatment, and prognostic significance. Neurology. 1992;42:1181-1184.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Barman B, Bhattacharya PK, Wankhar B, Warjri SB, Beyong TMetastatic Breast Carcinoma Associated with Numb Chin Syndrome.JCR 2014;4:520-523 |
|
Barman B, Bhattacharya PK, Wankhar B, Warjri SB, Beyong TMetastatic Breast Carcinoma Associated with Numb Chin Syndrome.JCR [serial online] 2014[cited 2026 May 21];4:520-523. Available from: http://www.casereports.in/articles/4/2/Metastatic-Breast-Carcinoma-Associated-with-Numb-Chin-Syndrome.html |

|
|
|
|
|