|
|
|
|
|
Primary Musculoskeletal Hydatid Mimicking a Neoplasm
|
|
|
1Chetana R. Ratnaparkhi, 1Kajal R. Mitra, 1Amay M. Kulkarni, 2Debashish R. Barick, 2Amit N. Nemade
From the 1Department of Radiodiagnosis & Imaging and 2Department of Orthopedics, NKP Salve Institute of Medical Sciences and Lata Mangeshkar Hospital, Digdoh Hills, Nagpur. Maharashtra, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Chetana R. Ratnaparkhi
Email: chetanaratnaparkhi@gmail.com
|
|
|
|
|
|
|
|
|
Received:
20-AUG-2014 |
Accepted:
04-OCT-2014 |
Published Online:
05-NOV-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Causative organism for hydatid disease in humans is Echinococcus granulosus and few other types of tapeworm. In a life cycle of Echinococcus, humans are accidental hosts who get infected by ingestion of the eggs of the parasite containing oncosphere, from close contact with infected animals or from the ingestion of contaminated food or water. Most common site of involvement in humans is liver, followed by the lungs. Musculoskeletal involvement in hydatid disease is mostly secondary to liver or lung hydatid. Primary musculoskeletal involvement is a rare manifestation of hydatid disease. We report herein a case of primary hydatid disease involving pubic bone, which is a rare site and only few cases of pubic bone hydatid cysts are reported in literature. Imaging, especially Magnetic Resonance Imaging, plays a pivotal role in reaching the diagnosis as in our case and helps in differentiating from other pathologies. |
|
|
|
|
|
Keywords :
|
Magnetic Resonance Imaging, Echinococcus, Liver, Parasites, Animals, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff0c00060000003f03000001000c00 6go6ckt5b5idvals|385 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Hydatid disease is a zoonosis, distributed worldwide and in few countries such as Mediterranean region, Central Asia, North and East Africa, Australia, South America and Middle East, it is endemic [1]. Hydatidosis can affect any organ in the body with affinity for hepatic and pulmonary systems. Primary musculo-skeletal hydatid cyst is exceptionally rare and is seen in 0.7-3% cases of hydatidosis [2]. Diagnoses of musculoskeletal hydatid disease on clinical grounds are difficult and mostly imitate neoplasm. Radiograph shows expansile lytic lesion with significant surrounding soft tissue component, making diagnosis difficult as these features mimic aggressive neoplastic lesion. However, MRI features of hydatid disease are unique and seldom require confirmation by serological markers or fine needle aspiration. We present a rare case of primary bone hydatid involving pubic bone with extension into groin and pelvis.
Case Report
A 62 year old man came with complaints of dull aching pain and gradually increasing lump in left groin extending to the upper thigh, of two years duration. Patient had difficulty in walking since two years. Vital parameters of the patient were stable. Patient had an episode of myocardial ischemia one year back. On local examination, a mass measuring approximately 7x1.5 cm was seen on anterior aspect of left thigh having well defined margins and smooth surface. It was soft in consistency. Routine blood investigations including total leukocyte counts and erythrocyte sedimentation rate (ESR) were within normal limits. Considering the history, age of the patient and clinical findings; diagnosis of malignant soft tissue lesion, i.e., sarcoma was kept. Patient was subjected to imaging for confirmation and extent of lesion.
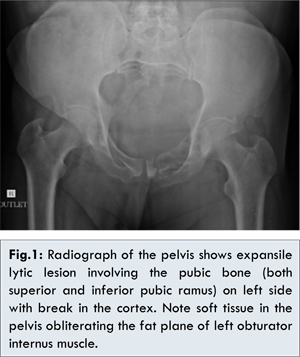
Radiograph of pelvis with both hips showed expansile lytic lesion involving the superior and inferior pubic rami on left side and part of the acetabulum [Fig.1]. At few places the cortex was broken. No periosteal reaction was seen. A large soft tissue was seen inside the pelvis, obliterating the obturator internus fat plane. External soft tissue lesion was not seen on radiograph.
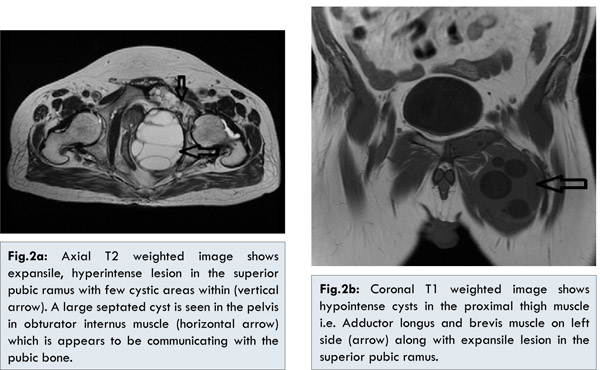
MRI of pelvis including thigh showed irregular cortical outline and heterogeneous altered signal intensity areas in the pubic rami on left side showing few well defined hyperintense areas on T2 weighted and short tau inversion recovery (STIR) images ( i.e., cysts) and distinct hypointense foci on all pulse sequences representing bone remnants. Two well defined lesions containing multiple cystic areas appearing hyperintense on T2 weighted images and STIR are seen one of size 9.8x8x7.5 cm in the obturator internus muscle and another of size 8.5x7.5x5.5 cm involving pectineus, adductor longus and brevis muscle on left side [Fig.2A,2B]. These two lesions in the muscles appear to be communicating with the superior pubic ramus. Based on these imaging findings diagnosis of hydatid disease of superior pubic ramus with extensions into adjoining muscles in the pelvis and medial thigh, was made. Curettage of left SPR was done with excision of pelvic cyst through peritoneal approach and thigh cyst via femoral triangle.
Echinococcosis in humans is commonly caused by Echinococcus granulosus [3]. Humans are infected by the ingestion of contaminated food or water containing eggs of the parasite. After the outer capsules of the eggs has been ingested, oncosphere enter the branch of portal vein and these oncosphere are lodged in the hepatic vasculature while some pass through the capillary bed and lodge in the lungs. Very few pass through the pulmonary circulation and infect other organs via hematogenous route.
Musculoskeletal involvement is generally secondary to lung or liver disease. Primary musculoskeletal hydatidosis is a rare occurrence as repetitive motion and high lactic acid levels make it less favorable site for the parasite [4]. Commonly affected bones are vertebrae (50%) followed by pelvis (25%) and long bones (15-25%) [5]. Patients with hydatid disease are generally asymptomatic till the pathological fracture or neurovascular impingement by the cyst or secondary infection within the cyst draw patients’ attention [6]. Considering the chronicity of illness, patients are mostly diagnosed as having neoplastic etiology as in our case.
Three distinct radiographic stages are seen in skeletal hydatid [7]. The first stage is a stage of microvesicular infiltration of embryos in the bone resulting in destruction by mechanical pressure and local necrosis by impairment of the blood supply. Microvesicles grow along the line of least resistance producing large vesicles that invade and replace the medullary cavity. These cysts enlarge and later produce cystic spaces giving multilocular appearance. In initial stages, an ill-defined, multilocular, lucent area is seen in the epiphysis without periosteal reaction and clear demarcation from the normal bone. Later, well defined cystic areas become evident and cysts coalesce resulting in loss of bone, resembling a lattice type of trabecular pattern. Pathological fractures are known complication in first stage. Second stage, is a stage of superadded infection causing an inflammatory osteitis, reflected by trabecular thickening, bone loss and hyperostosis. Third stage, a stage of abscess formation, occurs after cortical extension into the adjacent soft tissues which appear as cystic lesions of variable sizes and may calcify over a period. Our case presented in third stage.
Imaging, especially MRI has established role in diagnosing the hydatid disease and resolving clinical dilemma [8]. Conventional radiographs may lead to erroneous impression of neoplastic etiology. Differential diagnoses on radiographs include tuberculosis, simple or aneurysmal bone cyst, giant cell tumors, malignant fibrous histiocytoma, chondrosarcoma and myeloma [9]. Computed tomography (CT) and MRI are considered as imaging modality of choice for hydatid cyst. Bone changes in hydatid cyst and its extent are best evaluated by Computed Tomography than any other imaging modality. Magnetic Resonance Imaging, because of its excellent soft tissue resolution is considered as the gold standard for diagnosis of hydatid cyst [7]. Both T1 and T2 weighted images show excellent intralesional morphology, i.e., multiple daughter cysts embedded in a large cystic lesion. Extension of the cyst into adjacent soft tissues and marrow changes are best evaluated with MRI [9].
Bony pelvis is often difficult location for complete excision and most of the time, patients land up with subtotal excision of hydatid cysts. Preoperative diagnosis and precise mapping of extensions of the lesion are helpful in operative planning.
Conclusion
Imaging modalities especially MRI plays important role in reaching the diagnosis of primary musculo-skeletal hydatidosis and defining extent of lesions. MRI of hydatid cyst has hallmark features leading to precise diagnosis, thereby obviating the need for serological tests and fine needle aspiration.
References
- García-Díez AI, Ros Mendoza LH, Villacampa VM, Cózar M, Fuertes MI. MRI evaluation of soft tissue hydatid disease. Eur Radiol. 2000;10(3):462-466.
- Tatari H, Baran O, Sanlidag T, Göre O, Ak D, Manisali M, et al. Primary intramuscular hydatosis of supraspinatus muscle. Arch Orthop Trauma Surg. 2001;121(1-2):93-94.
- Jain S, Chopra P. Cystic Echinococcosis of the Pelvic Bone with Recurrences: A Case Report: Korean J Parasitol. 2011;49(3):277–279.
- Tatari H, Baran O, Sanlidag T, Göre O, Ak D, Manisali M, et al. Primary intramuscular hydatosis of supraspinatus muscle. Arch Orthop Trauma Surg. 2001;121(1-2):93-94.
- Calvo AM, Cires JM, Monton S, Sarasibar H, Lasanta P, Artazcoz FJ. Inguinal tumor: a rare occurrence of hydatid disease. A case report. A Sist Sanit Navar. 2007;30(3):475-479.
- Patond KR, Srivastava SK, Kumar N. Musculoskeletal Hydatidosis. India Pract. 1991;54:299-302.
- Wlner D. Radiology of bone tumours and allied disorders, 4th edition. WB Saunders:1982; 1144-1179.
- Fahl M, Haddad FS, Huballah M, Kana’an S, Husheimi I, Azizi T. Magnetic resonance imaging in intradural and extradural spinal echinococcosis. Clin Imaging. 1994;18(3):179-183.
- Dhungel K, Ahmad K, Sah PL, Gupta MK, Rauniyar RK, Sajid Ansari A, et al. Primary Intrapelvic Hydatid Cyst Presenting with Urinary Retention. Journal of Case Reports. 2012;2(2):100-103.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
R. Ratnaparkhi C, R. Mitra K, M. Kulkarni A, R. Barick D, N. Nemade APrimary Musculoskeletal Hydatid Mimicking a Neoplasm.JCR 2014;4:424-427 |
|
R. Ratnaparkhi C, R. Mitra K, M. Kulkarni A, R. Barick D, N. Nemade APrimary Musculoskeletal Hydatid Mimicking a Neoplasm.JCR [serial online] 2014[cited 2026 May 21];4:424-427. Available from: http://www.casereports.in/articles/4/2/Primary-Musculoskeletal-Hydatid-Mimicking-a-Neoplasm.html |

|
|
|
|
|