Introduction
The term Rosai-Dorfman disease is now commonly applied to cases of sinus histiocytosis with massive lymphadenopathy (SHML) that manifests with isolated extra nodal involvement. This is a rare disease and isolated involvement of the paranasal sinuses is reported only in a few cases in literature [1].
Sinus histiocytosis with massive lymphadenopathy was first described as a distinct clinicopathological entity by Rosai and Dorfman [2]. This disease commonly affects children and young adults. The characteristic presenting features are painless cervical lymphadenopathy, fever, elevated erythrocyte sedimentation rates, leukocytosis and neutrophilia. The disease has a benign clinical course and spontaneous remission occurs in most cases. Recurrences have been reported in some cases.
Lymph node groups other than cervical may be involved and involvement of extra nodal sites is not uncommon.
Case Report
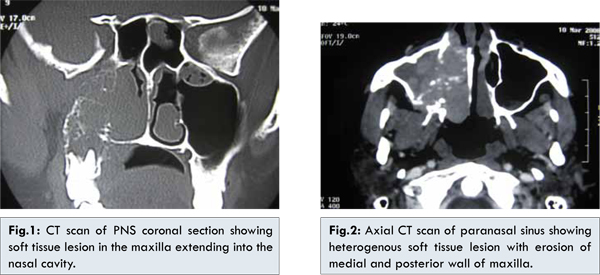
45 year old female presented with progressive right sided nasal obstruction and intermittent nasal bleeding of 3 months duration. There was no history of fever, ear block or headache. On examination irregular fleshy mass was seen in the right nasal cavity. The mass had an irregular surface and was bleeding on touch. There was no significant cervical lymphadenopathy. Diagnostic nasal endoscopy was done which showed an irregular mass occupying the right nasal cavity abutting the nasal septum. The mass was arising from the middle meatus. Nasopharynx was free. There was no parasthesia over the face or loosening of teeth. Hematological parameters were normal except an elevated ESR. CT scan with contrast showed an enhancing mass involving the right maxillary antrum extending to the right nasal cavity. Medial and posterior wall of the maxillary sinus was eroded [Fig.1,2].
Patient underwent an endoscopic medial maxillectomy and the mass was excised. The mass was delineated all around. When the mass was dissected from the posterior wall of maxillary sinus bleeding was encountered from the internal maxillary artery which was cauterized. The mass was excised in toto and sent for histopathological examination. The histopathology showed large pale cells with enlarged irregular nuclei, lymphocytes and plasma cells with fragments of fibrous tissue and calcific debris. Lymphophagocytosis was rare. S-100 stain was positive. These features were consistent with Rosai-Dorfman disease. The patient recovered well post-operatively and is on regular follow up [Fig.3] There is no recurrence of disease after 2 years.
Discussion
Rosai-Dorfman disease is the name given to sinus histiocytosis with massive lymphadenopathy. It is a disease which predominantly affects children and young adults. Most common presentation is with massive painless cervical lymphadenopathy, which in most cases is bilateral. Involvement of other lymph node groups is also common. However, in our patient there was no significant lymphadenopathy. Other clinical features include fever, weight loss, nasal discharge or obstruction and tonsillitis [3]. In over 50% cases there is extranodal involvement [4]. The most common extranodal sites involved are skin, soft tissue, upper respiratory tract, bone, eye and retro-orbital tissue. Other reported sites include urogenital tract, gastrointestinal tract, breast, liver, pancreas and lungs. CNS lesions can present clinically and radiologically as a menigioma. Involvement of paranasal sinus is very rare. Paranasal sinus involvement has been described in a few cases in literature [5,6]. Laboratory findings in this condition is non-specific. Leukocytosis and elevated ESR have been reported in most cases. Normocytic/normochromic and autoimmune hemolytic anemia with elevated serum ferritin has been reported in some cases. Histologically the disease must be differentiated from Langerhans cell histiocytosis, infectious and lymphoproliferative disorders as well as sinus hyperplasia. S-100 positivity can usually distinguish from these conditions.
Our patient is a 45 year old female patient who presented with isolated disease of the right maxillary sinus. The disease had eroded posterior wall of maxilla with involvement of the pterygopalatine fossa which is a rare phenomenon. Clinically the patient presented with complaints of nasal obstruction and epistaxis. The clinical picture along with the radiological feature of bony erosion led us to a clinical diagnosis of sinonasal malignancy. Extranodal Rosai-Dorfman disease is difficult to diagnose clinically and most often diagnosis is made on histopathological examination. The disease can mimic other disease and a high index of clinical suspicion is needed in diagnosis of these cases.
In majority of the cases the disease runs a benign course and is self-limiting. In some cases it can have remissions and exacerbations. No specific treatment has been advocated for this essentially self-limiting disease, which has a good prognosis [7]. Surgical treatment of resectable lesions gives complete remission. Debulking is indicated in patients with vital organs or airway compromise [8]. Prolonged course of low dose steroids is useful in reducing the nodal size [9]. Long-term follow-up of the patient is beneficial in detecting recurrence and/or any other site involvement and its appropriate management.
Conclusion
Involvement of the paranasal sinuses as encountered by us is an extremely rare presentation of Rosai-Dorfman disease. The diagnosis is primarily a histopathological one and confirmation is with gamma globulin estimation and S-100 positivity.
References
- Wright DH, Richards DB. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): report of a case with widespread nodal and extra nodal dissemination. Histopathology 1981;5:697-709.
- Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy; a newly recognized benign clinicopathological entity. Arch Pathol 1969;87:63-70.
- Sanchez R, Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy; as analysis of 113 cases with special emphasis on its extranodal manifestations. Lab Invest 1977;36:349-350.
- Goodnight JW, Wang MB, Sercarz JA, Fu YS. Extranodal Rosai-Dorfman disease of the head and neck. Laryngoscope; 1996;106(3 Pt 1):253-256.
- Hagemann M, Zbären P, Stauffer E, Caversaccio M. Nasal and paranasal sinus manifestation of Rosai-Dorfman disease. Rhinology; 2005;43(3):229-232.
- Gregor RT, Ninnin D. Rosai-Dorfman disease of the paranasal sinuses. J Laryngol Otol 1994;108:152-155.
- Foucar E, Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy: current status and future directions. Arch Dermatol 1988; 124:1211-1214.
- Pulsoni A, Anghel G, Falcucci P, et al. Treatment of sinus histiocytosis with massive lymphadenopathy: report of a case and literature review. Am J Hematol 2002;69:69-71.
- Oka M, Kamo T, Goto N, et al. Successful treatment of Rosai-Dorfman disease with low-dose oral corticosteroid. J Dermatol 2009;36:237-240.