|
|
|
|
|
Small Bowel Obstruction due to an Incarcerated Obturator Hernia
|
|
|
pillola cialis effetti tadalafil teva
From the Department of Surgery, Caboolture Hospital, Caboolture, Queensland, Australia. |
|
|
|
|
|
Corresponding Author:
|
Dr. D. Mehanna
Email: dmehanna@hotmail.com
|
|
|
|
|
|
|
|
|
Received:
09-APR-2014 |
Accepted:
18-NOV-2014 |
Published Online:
05-DEC-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Obturator hernia is a rare but important hernia tending to affect elderly females in whom diagnosis is usually difficult given the absence of specific signs and symptoms. This is a case report of a 78 year old female who presented with recurrent small bowel obstruction secondary to an obturator hernia in which a laparotomy was performed. The hernial defect was plugged with prolene mesh and the hernial opening closed with prolene sutures. |
|
|
|
|
|
Keywords :
|
Hernia, Small Intestine, Laparotomy, Hernia, Intestinal Obstruction, Sutures, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff3c00060000001903000001001d00 6go6ckt5b5idvals|397 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Obturator hernia is the most common of the rare pelvic floor hernias with documented incidence ranging from 0.7-1% of all hernias [1]. It is an important surgical entity as it has non-specific signs and symptoms making it difficult to diagnoses and tends to occur in the vulnerable elderly population. We present a case of an incarcerated obturator hernia as a reminder that unless a high index of suspicion is held, the diagnosis may be missed.
Case Report
A 78 year old female nursing home resident presented with a several day history of vomiting, abdominal pain and distension. She had a background of Parkinson’s disease, transient ischemic attacks, epilepsy, hypertension, gastroesophageal reflux disease, laparoscopic cholecystectomy and a known cerebral aneurysm. Her medications included clopidogrel. She had presented to another hospital in recent weeks in a similar fashion but improved with conservative management.
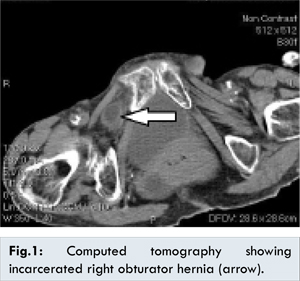
On examination the patient was confused, dehydrated and cachectic but afebrile. Her abdomen was soft but distended with no hernias palpable. Digital rectal examination was unremarkable. The patient was subsequently resuscitated. Full blood count, coagulation profile and electrolytes were within normal limits. Abdominal films showed slightly prominent loops of small bowel however not diagnostic for a small bowel obstruction. A computed tomography revealed the presence of an incarcerated right obturator hernia with dilated loops of small bowel [Fig.1]. The patient was examined for evidence of the Howship-Romberg sign, which was not detected.
After consultation with a haematologist, platelet cover was organised and our patient was taken to theatre. A midline laparotomy was performed with minimal bleeding encountered. Intra-operatively, dilated loops of small bowel were found proximal to a knuckle of terminal ileum 10 centimetres from the ileocecal junction caught in the right obturator canal as a Richter’s hernia. The segment of affected small bowel was found to be bruised but viable [Fig.2]. The abnormally wide opening of the obturator canal was noted with surrounded bruising [Fig.3]. The hernial defect was closed with a prolene mesh plug and the opening closed with 2/0 prolene interrupted sutures. The patient made a slow but steady recovery and was discharged on the 7th post-operative day.
Discussion
Obturator hernia was first described 1724 by Arnaud de Ronsil and Henry Obre first performed a successful repair in 1851[1]. It has been reported to account for 0.07-1.0% of all hernias and 0.2-1.6% of all small bowel obstruction [1-5]. Obturator hernias occur most commonly in elderly, debilitated women because of the loss of protective fat in the obturator canal, the broader pelvis and wider canal in women [1-6]. Herniation is most common on the right as the sigmoid colon tends to prevent it on the left [5,7].
Three stages of the development of an obturator hernia have been described by Gray et al. The first stage is the entrance of preperitoneal tissue into the pelvic orifice of the obturator canal, while the second stage involves the development of a dimple in the peritoneum overlying the canal. The third stage is the onset of symptoms produced by entrance of an organ which may contain small bowel, large bowel, omentum, fallopian tube or appendix [1,8].
Greater than 90% of patients with an obturator hernia present with intestinal obstruction that causes pain, nausea and vomiting with one third of patients having a previous history of small bowel obstruction as was the case with our patient [2,8]. Obstruction is usually partial due to the high frequency (41-100%) of Richter’s herniation of small bowel into the obturator canal [5,9]. The Howship-Romberg sign, pain extending down the medial aspect of the thigh caused by irritation of the anterior division of the obturator nerve by the hernial sac and its contents is present in 12.5-65% of patients [1,2,3,5,8]. Various imaging modalities have been used to aid diagnosis with CT scan being the most useful [3,5,9].
A variety of techniques have been advocated for its repair including an abdominal approach, retropubic approach, obturator approach, inguinal approach and more recently, the laparoscopic approach [4,6,10]. The abdominal approach via a low midline incision is most commonly favoured, as the advantages of this approach include establishing a diagnosis, avoidance of obturator vessels, better exposure of the obturator ring, and facilitation of bowel resection, if necessary. Many authors prefer a simple closure of the hernial defect with one or more interrupted sutures as it leads to an acceptable recurrence rate of less than 10% [7,9]. The defect can also be closed by synthetic mesh. The laparoscopic approach is an alternative to diagnose, reduce and repair an obturator hernia in selected cases. Both transabdominal and extraperitoneal approaches have been described.
In summary, obturator hernia is a rare condition that generally affects elderly females with symptoms of small bowel obstruction. Clinical signs specific to this condition may not be present and are usually not sought out unless the diagnosis has been specifically considered. Early diagnosis can be facilitated by the use CT scanning. Both open and more recently laparoscopic approaches have been described for its repair.
References
- Agarwal D, Sharma G, Kumar N, Rao J. Intestinal Obstruction due to obturator hernia (a rarest presentation). Ind J Surg. 2013;75 (Supp 1):S388-S390.
- Kulkarni S, Punamiya A, Naniwadekar R, Janugade H, Chotai T, Singh V, et al. Obturator hernia: a diagnostic challenge. Int J Surg Case Reports. 2013;606-608.
- Lai CC, Huang AH, Liao WH, Lin SH. Usefulness of CT for differentiating between obturator hernia and other causes of small bowel obstruction. Postgrad Med J. 2013;89:729-730.
- Lynch N, Corrigan M, Kearney D, Andrews E, et al. Successful laparoscopic management of an incarcerated obturator hernia. J Surg Case Rep. 2013;7:1-3.
- Kammori M, Mafune K, Hirashima T, Kawahara M, Hashimoto M, Ogawa T, et al. Forty-three cases of obturator hernia. Am J Surg. 2004;187:549-552.
- Deeba S, Purkayastha S, Darzi A, Zacharakis E. Obturator hernia: a review of the laparoscopic approach. J Min Access Surg. 2011;7:201-204.
- Karsaki T, Nomura Y, Tanaka N. Long-term outcomes after obturator hernia repair: retrospective analysis of 80 operations at a single institution. Hernia. 2014;18(3):393-397.
- Gray SW, Skandalakis JE, Soria RE, Rowe JS Jr. Strangulated obturator hernia. Surgery. 1974;75:20-27.
- Mantoo SK, Mak K, Tan TJ. Obturator hernia: diagnosis and treatment in the modern era. Singapore Med J. 2009;50:866-870.
- Lobo DN, Clarke DJ, Barlow AP. Obturator hernia: a new technique for repair. J R Coll Surg Edinb. 1998;43:33-34.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Fick A, Mehanna D, Dissanayake T, Mehanna PSmall Bowel Obstruction due to an Incarcerated Obturator Hernia.JCR 2014;4:471-473 |
|
Fick A, Mehanna D, Dissanayake T, Mehanna PSmall Bowel Obstruction due to an Incarcerated Obturator Hernia.JCR [serial online] 2014[cited 2026 May 27];4:471-473. Available from: http://www.casereports.in/articles/4/2/Small-Bowel-Obstruction-due-to-an-Incarcerated-Obturator-Hernia.html |

|
|
|
|
|