|
|
|
|
|
Syndrome of Inappropriate Anti-diuretic Hormone Secretion and Pregabalin – a Critical Alert on a Potentially Reversible Side-effect
|
|
|
amlodipin 5 mg amlodipin teva
From the Department of General Medicine, Pondicherry Institute of Medical Sciences,
Pondicherry-605014, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Sudhagar Mookkappan
Email: drsudhagar_ms@yahoo.in
|
|
|
|
|
|
|
|
|
Received:
18-AUG-2014 |
Accepted:
24-SEP-2014 |
Published Online:
25-OCT-2014 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is the commonest cause of euvolemic hyponatremia. Several drugs are known to cause this syndrome. Pregabalin, a drug now used widely for a number of neurologic disorders, may cause hyponatremia secondary to salt wasting nephropathy. However, SIADH induced by pregabalin has been reported very infrequently in the literature. We report a case of hyponatremia in a patient started on pregabalin recently, who fulfilled criteria for SIADH and rapidly reversed on discontinuation of the drug. Awareness of this complication will help the clinician to diagnose and treat new onset hyponatremia in patients started on pregabalin. |
|
|
|
|
|
Keywords :
|
Hyponatremia, Nervous System Diseases, Inappropriate ADH Syndrome, Vasopressins, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1fffcff050000003c03000001000700 6go6ckt5b5idvals|381 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Hyponatremia, often defined as serum sodium less than 130 mmol/L, is the most common electrolyte disturbance among hospitalized patients [1,2]. The syndrome of inappropriate anti-diuretic hormone secretion (SIADH), first reported by Bartter and Schwartz in 1967, is the most common cause of euvolemic hyponatremia [3]. Causes of SIADH include malignant diseases (e.g., carcinoma, lymphomas, sarcomas), pulmonary disorders (e.g., pneumonia, asthma), central nervous system disorders (e.g., meningitis, stroke, head trauma), and a number of medications [1]. We report a case of drug induced SIADH due to pregabalin commonly used for neuropathic pain. Although pregabalin induced hyponatremia due to salt wasting nephropathy has been described, SIADH as the underlying mechanism of hyponatremia due to pregabalin has been reported only rarely.
Case Report
A 55-year-old male presented with nausea and hiccups. Two weeks before this he was started on pregabalin 75 mg once daily for his neuropathic pain secondary to L4,L5 radiculopathy. He was neither a diabetic nor a hypertensive. There was no past history of hypothyroidism or coronary artery disease. Apart from pregabalin, he was not on any medications. Physical examination was normal. Clinically he was euvolemic as evidenced by absence of pedal edema, a normal jugular venous pressure, clear chest and absence of signs of dehydration. His complete blood counts, blood sugars, urea, creatinine and uric acid were normal. His serum sodium was 108 meq/L and potassium 4.2 meq/L, serum osmolarity 260 mosm. Urinary sodium was 60 meq/L and potassium 80 meq/L and urine osmolarity 280 mosm. His thyroid profile, serum cortisol, chest X-ray, ECG and 2D echocardiogram were normal. Hence criteria for SIADH were fulfilled. Moreover, since he was not on any other medication and had no evidence of infection or malignancy, we presumed that SIADH was secondary to pregabalin. Further evidence for this was obtained by the prompt normalization of sodium within 3 days of discontinuing pregabalin. Patient improved clinically and biochemically after stopping pregabalin. He came for follow up after two weeks and his serum sodium was 132 mmol/L.
Discussion
Hyponatremia is the most frequent electrolyte disorder [1,2] and SIADH accounts for approximately one-third of all cases [3]. Antidiuretic hormone (ADH), also known as Arginine vasopressin (AVP) is secreted from the posterior pituitary gland in response to an increased plasma sodium concentration. It increases cellular permeability to water in the distal tubule and collecting duct of the nephron, leading to water reabsorption by the kidney [4,5].
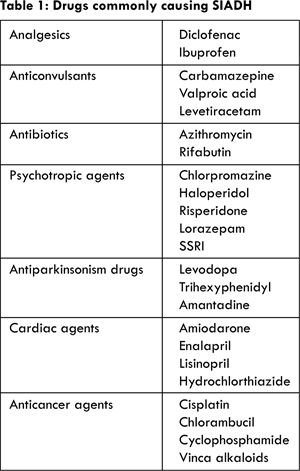
SIADH is characterized by either a sustained release of ADH in the absence of any stimulus, or by enhanced action of ADH on the kidneys [6]. Increased ADH activity in kidneys impairs ability to dilute urine resulting in decreased excretion of ingested water and a highly concentrated and low volume urine [4,5]. In this setting unrestricted fluid intake leads to hypotonicity of plasma and hyponatremia results. Usually SIADH patients have euvolemic status because excess water gets evenly distributed across all body compartments [5]. The causes of SIADH include malignant disease, pulmonary disorders, central nervous system causes and drugs [1]. Drugs that are commonly implicated to cause SIADH are listed in table 1. In order to diagnose SIADH it is important to ascertain the euvolemic status of the patient, both clinically and by laboratory measurements.
We describe a case of drug induced SIADH due to pregabalin. Pregabalin is an analog of the neurotransmitter gamma-aminobutyric acid that has analgesic, anticonvulsant and anxiolytic properties [7]. It is now widely used for neuropathic pain (diabetic, post herpetic and neuropathy associated with spinal cord injury), adjunctive therapy in partial seizures, anxiety disorders and fibromyalgia. The common side effects of pregabalin are dizziness and somnolence due to central nervous system disturbances [8]. Other dose dependent side effects reported with pregabalin include peripheral edema and weight gain [7,9].
Hyponatremia has been reported as an uncommon side effect of pregabalin. Both salt wasting nephropathy and SIADH have been described, resulting in this infrequent adverse effect [10,11]. Our patient had euvolemic hyponatremia with low serum osmolarity, high urine sodium and normal thyroid function and cortisol, all fitting the criteria for SIADH [1]. Clinical and laboratory features of salt wasting nephropathy and SIADH overlap significantly, distinction being made possible only by euvolemia and improvement with fluid restriction in the latter [12,13]. Our patient had a normal central venous pressure and improved with fluid restriction.
We used the Naranjo algorithm to objectively ascertain that pregabalin resulted in the adverse event in this patient [14]. Drugs induce SIADH by either increasing the sensitivity of the nephron to ADH (chlorpropamide) or augmenting the production of ADH centrally (antipsychotics, antidepressants and vinca alkaloids). Certain drugs like cyclophosphamide and carbamazepine utilize both mechanisms [5]. Since most actions of pregabalin occur via interactions within the central nervous system, it seems logical to hypothesise that pregabalin induces SIADH by increasing the secretion of ADH form the pituitary. However, more case reports and large scale randomized trials are required to test this hypothesis.
Conclusion
SIADH, particularly due to drugs is becoming an increasingly common cause for hyponatremia. Analysis of available literature and our case report indicates that pregabalin may cause hyponatremia by inducing salt wasting nephropathy as well as SIADH. Clinicians must be aware of this possibility since withdrawal of the drug results in rapid correction of hyponatremia due to SIADH.
References
- Ellison DH, Berl T. The syndrome of inappropriate antidiuresis. N Engl J Med. 2007;356(20):2064-2072.
- Palmer BF, Gates JR, Lader M. Causes and management of hyponatremia. Ann Pharmacother. 2003;37:1694-1702.
- Bartter FC, Schwartz WB. The syndrome of inappropriate secretion of antidiuretic hormone. Am J Med. 1967;42:790-806.
- Rose BD. Causes of the SIADH. In: Rose BD, ed. UpToDate [electronic database]. Waltham, MA, 2007.
- Foote EF. Syndrome of inappropriate antidiuretic hormone secretion and diabetes insipidus. In: Tisdale JE, Millder DA (eds). Drug-induced diseases, prevention detection and management. Bethesda, MD: American Society of Health-System Pharmacists; 2005:611-624.
- Spigset O, Hedenmalm K. Hyponatremia and the syndrome of inappropriate antidiuretic hormone secretion (SIADH) induced by psychotropic drugs. Drug Saf. 1995;12:209-225.
- Page RL, Cantu M, Lindenfeld J, Hergott LJ, Lowes BD. Possible heart failure exacerbation associated with pregabalin: case discussion and literature review. J Cardiovasc Med 2008;9(9): 922-925.
- De Smedt RHE, Jaarsma T, van den Broek SAJ, Haaijer-Ruskamp FM. Decompensation of chronic heart failure associated with pregabalin in a 73-year-old patient with post-herpetic neuralgia: a case report. Br J Clin Pharmacol. 2008;66(2):327-328.
- Murphy N, Mockler M, Ryder M, Ledwidge M, McDonald K. Decompensation of chronic heart failure associated with pregabalin in patients with neuropathic pain. J Card Fail. 2007; 13(3):227-229.
- Arnon Blum, Claudia Simsolo, Imad Tatour. Hyponatremia and Confusion Caused by Pregabalin. IMAJ. 2009;11:699-700.
- Haddad F, Jammal M, Chehwane D, Abi Saleh R, Koussa S. Gait instability revealing a syndrome of inappropriate antidiuretic hormone secretion associated to pregabalin. Rev Med Interne. 2012;33(11):e49-51.
- Upadhyay UM & Gormley WB.Etiology and management of hyponatremia in neurosurgical patients. J Intensive Care Med. 2012;27:139-144.
- Momi J, Tang CM, Abcar AC, Kujubu DA, Sim JJ. Hyponatremia-what is cerebral salt wasting? Perm J. 2010;14:62-65.
- Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239-245.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Mookkappan S, Basheer A, Iqbal NSyndrome of Inappropriate Anti-diuretic Hormone Secretion and Pregabalin – a Critical Alert on a Potentially Reversible Side-effect.JCR 2014;4:408-411 |
|
Mookkappan S, Basheer A, Iqbal NSyndrome of Inappropriate Anti-diuretic Hormone Secretion and Pregabalin – a Critical Alert on a Potentially Reversible Side-effect.JCR [serial online] 2014[cited 2026 May 12];4:408-411. Available from: http://www.casereports.in/articles/4/2/Syndrome-of-Inappropriate-Anti-diuretic-Hormone-Secretion-and-Pregabalin.html |

|
|
|
|
|