6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff34f8050000003003000001000100
6go6ckt5b5idvals|370
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Laryngeal web is a rare anomaly, mostly congenital in origin with incidence of 1:10,000. Laryngeal web can also be acquired by iatrogenic trauma (like intubation), infection (tuberculosis) and chronic aspiration. Laryngeal web may be asymptomatic or incidentally reported after failed intubation (due to web) during anaesthesia. Treatment of laryngeal web is dilation, endoscopic excision or laser excision These cases pose a challenge to the anaesthesiologists in not only difficult intubation but also problems like fire hazards due to CO2 laser and/or bronchospasm. We report our experience in a case of unanticipated laryngeal web posted for unilateral arytenoidectomy and cordectomy by CO2 laser.
Case Report
A 9 year old child ASA-2, weighting 20 kg presented with bilateral abductor vocal cord palsy following post tracheostomy decannulation 1 year back. Past history revealed that one year back patient was admitted in ICU due to head injury. He was intubated with endotracheal tube and put on mechanical ventilation. After 10 days tracheostomy was done. Gradually patient was weaned from ventilator and decannulation was done after 3 month of admission. About 4 month after decannulation patient developed horseness of voice, stridor and difficulty in breathing, the severity of which increased gradually.
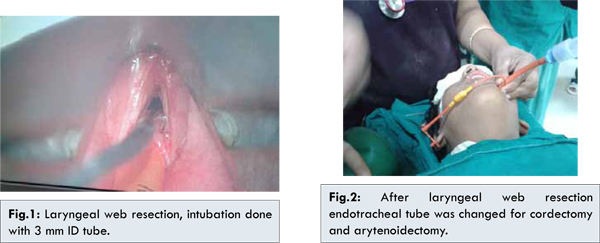
Patient was posted for unilateral arytenoidectomy and cordectomy by CO2 laser. Routine pre-operative evaluation and lab investigations were within normal limits. Indirect laryngoscopy suggested bilateral abductor vocal cord palsy and no other abnormality. In operating room all standard monitors were attached. Patient was premedicated with glycopyrolate 0.04 mg/kg, fentanyl 2 µg/kg. Induction was done by propofol 2 mg/kg. Bag and mask ventilation established then succinylcholine 2 mg/kg was given. IPPV was given for 60 secs. Endotracheal intubation was attempted with 5 mm ID red rubber endotacheal tube wrapped with aluminium foil, but tube could not be negotiated through glottic opening. Then several attempts were made plain 5.0 mm, 4.5 mm, 4.0 mm ID red rubber endotracheal tube, but intubation was unsuccessful. Surgeon decided to do endoscopic examination. During endoscopy, patient was ventilated by jet ventilation and maintenance by repeated dose of propofol. Endoscopy revealed anterior and subglottic laryngeal web for which web excision was planned before cordectomy and arytenoidectomy. After endoscopic examination patient was oxygenated with bag and mask, and successfully intubated with 3.0 mm ID plain red rubber endotracheal tube. After confirmation of bilateral equal air entry and capnography, endotracheal tube was secured. Anaesthesia was maintained with oxygen, nitrous oxide and isoflurane and intermittent dose of atracurium 2 mg. Surgeon placed wet cotton pledgets around the tube for protection against laser burns to airway. The laryngeal web was excised with CO2 laser. For preventing fire intermittent apnea technique was used during web excision. After web excision endotracheal tube was replaced with 4.5 mm uncuffed endotracheal tube for adenoidectomy and cordectomy by direct laryngoscopy. Mitomycin was locally spread by surgeons after the procedure. The anaesthetic course was uneventful and patient extubated safely. The patient was discharged from hospital 1 week later.
Discussion
The cause of difficult intubation in our case was unexpected laryngeal web. The laryngeal webs are formed by thin transparent or thick fibrous membrane. Web may be congenital or acquired. The incidence of congenital laryngeal web has been estimated around 1 in 10,000 live births [1]. They may be associated with some syndrome like Digeorge syndrome, Velo cardio facial syndrome [2]. Laryngeal webs are mainly located at the level of vocal cord some being either sub or supraglottic. Majority of these lies anteriorly between the cords, only 1-2 % are located posteriorly [3]. The etiology of laryngeal web formation in our case was post-tracheostomy complication.
Laryngeal web are classified based on degree of airway obstruction (Cohen grading scale) [4]. Type I: < 35 % of airway obstruction, Type II: 35-50% of airway obstruction, Type III: 50-75% of airway obstruction, Type IV: 75-90% of airway obstruction. Our patient had type III of above classification.
Clinical presentation may vary from hoarseness of voice, stridor to croup, respiratory distress and dysphagia. Laryngeal web may be misdiagnosed as obstructive lung disease such as bronchial asthma or COPD especially when they are located subglottic [5]. Some patients remain asymptomatic and may present as unanticipated difficult intubation.
Airway management of laryngeal web is clinically same as management of subglottic stenosis. Different size tracheal tube should be kept ready during induction of anaesthesia. Further trauma to vocal should be avoided as trauma may cause further scarring and web formation. There are cases reported on web formation after intubation [6]. Patient who are asymptomatic do not require any treatment, other patient are managed by surgical division mainly by CO2 laser. Other treatment options are laryngeal knives, radiofrequency current, laryngeal microscissors, galvanocautery [7].
There are various endoscopic techniques for the treatment of bilateral abductor vocal cord palsy. Trans-oral arytenoidectomy and cordectomy are the most common method used for management. CO2 laser is the most appropriate for this with advantages of better haemostasis, minimal tissue handling. In our patient, surgeons planned for anterior cordectomy with arytenoidectomy by CO2 laser. Our patient did not have any airway obstruction so after induction of anaesthesia bag and mask ventilation was easily achieved. Endotracheal intubation with different sizes of red rubber endotracheal tube failed. After confirmation of laryngeal web by surgeons by endoscopic examination, endotracheal intubation was reattempted by 3 mm ID plain red rubber tube. We used red rubber tube because there are more chances of laser fire in PVC tubes. Aluminium foil wrapping was not possible because of use of smaller size tube so the surgeons placed wet cotton pledgets around the tube and intermittent apnea (JR circuit disconnected when CO2 laser fired) technique was used. After resection of web tube was replaced with 4.5 mm ID cuffed endotracheal tube and then cordectomy and arytenoidectomy was performed and then mitomycin was applied locally.
To conclude, preparedness for difficult airway management and working as a team with surgeons can avoid any disaster and leads to better outcome.
References
- Hannallah R, Rosales JK. Laryngeal web in an infant with tracheoesophageal fistula. Anesthesiology 1975;42(1):96-97.
- Miyamoto RC, Cotton RT, Rope AF, Hopkin RJ, Cohen AP, Shott SR, et al. Association of anterior glottic webs with velocardiofacial syndrome (chromosome 22q11. 2 deletion). Otolaryngol Head Neck Surg 2004;130:415-417.
- Chong ZK, Jawan B, Poon YY, Lee JH. Unsuspected difficult intubation caused by a laryngeal web. Br J Anaesth 1997;79(3):396-397.
- Cohen SR. Congenital glottis webs in children. A retrospective review of 51 patients. Ann Otol Rhinol Laryngol Suppl 1985;94 (suppl 121):2-16.
- Legasto AC, Haller JO, Giusti RJ. Tracheal web. Pediatr Radiol 2004;34(3):256-258.
- Kokkonouzis I, Mermigkis C, Psathakis K, Tsintiris K. Postintubation tracheal web. Journal of Bronchology 2005;12(4):271-272.
- Cummings CW. Otolaryngology-Head and Neck Surgery. London: CV Mosby, 1986.