|
|
|
|
|
Emphysematous Pyelonephritis
|
|
|
tadalafil generico mylan cialis generico in farmacia senza ricetta
Department of Emergency Medicine, The Mission Hospital, Durgapur, West Bengal - 713212, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Wasil Rasool Sheikh
Email: wasil.sheikh@hotmail.com
|
|
|
|
|
|
|
|
|
Received:
16-JAN-2015 |
Accepted:
13-MAR-2015 |
Published Online:
05-APR-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Emphysematous pyelonephritis is a gas-producing necrotizing bacterial infection that involves the renal parenchyma and perirenal tissue. We report a case of diabetes mellitus that presented to the emergency department with abdominal pain, decreased urine output and altered mental status and was diagnosed as emphysematous pyelonephritis with severe uro-sepsis. Early recognition in the emergency department prompted aggressive medical management followed by percutaneous drainage due to which patient was successfully treated. Early diagnosis and management is a key to the prognosis in emphysematous pyelonephritis. |
|
|
|
|
|
Keywords :
|
Abdominal Pain, Pyelonephritis, Sepsis, Kidney, Drainage, Diabetes Mellitus.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff0427060000008d03000001000600 6go6ckt5b5idvals|446 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Emphysematous pyelonephritis (EPN) is a severe, acute necrotizing infection with formation of gas in the collecting system, renal parenchyma and perirenal tissues. It is a potentially fatal infection with a variable clinical picture which ranges from mild abdominal pain to septic shock. It is mostly unilateral but is bilateral in 10% cases. Most of the cases are seen in diabetics, about 90% reported according to different series; obstructive uropathy is the other contributing factor in other cases [ 1, 2]. Computed tomography (CT) is the diagnostic radiological investigation. Escherichia coli is the most common causative pathogen isolated in urine or pus culture in nearly 70% of the reported cases [ 3]. Researchers have postulated that vigorous resuscitation and appropriate medical treatment should be followed by immediate nephrectomy [ 2, 4]. However, current advances in treatment allow patients to be treated with percutaneous drainage in combination with broad spectrum antibiotics [ 1, 5, 6].
Case Report
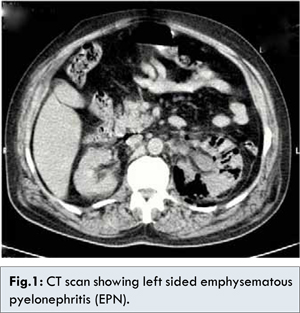
A 59 year old diabetic male patient was brought to the emergency department with chief complaints of left sided abdominal pain, mild abdominal distension, decreased urine output since 2 days and altered mental status since 1 day. Vitals on admission were HR=110/min, Temperature=97°F, BP=100/60 mm Hg, RR=35/min, SPO2=92% at room air, CBG=209 mg/dL. Examination revealed an ill appearing patient in altered mental status with tenderness in the left flank. Venous blood gas analysis showed severe metabolic acidosis (pH=7.30, HCO3=9.7, PCO2=19.9); complete blood count: Hb=12, TLC=15700/mm3 with 84% neutrophils, platelet count=0.60 lakhs/cumm, urea=97 mg%, creatinine=3.2 mg/dL, potassium=5.5 meq/L, procalcitonin > 75 ng/dL. Urine examination showed pus cells= 8-9/hpf, presence of bacteria, blood=2+, RBC=10-12/hpf. Ultrasound screening in the emergency department showed air shadow/artifacts in the left pelvi-calyceal system with features of mild hydronephrosis. Non-contrast CT abdomen was done which revealed gas in the left renal region, suggestive of left sided emphysematous pyelonephritis, Class 3a [Fig.1] according to Huang et al. classification.
The patient received intravenous fluids, antibiotics along with supportive care in the emergency department and was admitted in ICU with a diagnosis of emphysematous pyelonephritis and severe urosepsis. Ultrasound guided percutaneous nephrostomy was done from which air and pus were aspirated. Gram staining of nephrostomy aspirate revealed gram negative bacilli and culture showed E. coli. Appropriate antibiotics were given as per the culture and sensitivity reports. Insulin was added to control the diabetes and other supportive care was given. Patient started recovering clinically and was discharged for follow up in the urology department.
Discussion
Emphysematous pyelonephritis is a rare necrotizing infection of the upper urinary tract. 90% patients are diabetics. Female diabetic patients and left kidney are more commonly affected. Involvement of both kidneys is seen in 5% patients [ 7]. The most common pathogen is Escherichia coli (70%), followed by Klebsiella pneumoniae (29%) and Proteus. These bacteria ferment sugars within the urine producing gases including nitrogen, hydrogen, carbon dioxide, and oxygen [ 8].
Renal ultrasound can confirm the presence of EPN in approximately 80% of cases [9], whereas CT scan is 100% sensitive [4]. Thus, a CT scan is mandatory to diagnose EPN if the index of suspicion is high. The most recent CT classification of EPN by Huang et al. [ 1] describes the anatomical location of gas on CT scan. Class 1: Gas confined to the collecting system; Class 2: Gas confined to the renal parenchyma alone; Class 3a: Perinephric extension of gas or abscess; Class 3b: Extension of gas beyond the Gerota fascia; Class 4: Bilateral EPN or unilateral EPN with a solitary kidney.
Huang and Tseng et al. [ 1, 6] proposed certain therapeutic modalities based upon their radiological classification system. Localized emphysematous pyelonephritis (class 1 and 2) is confronted by antibiotic treatment, combined with CT-guided percutaneous drainage. For extensive EPN (classes 3 and 4) without signs of organ dysfunction, antibiotic therapy combined with percutaneous catheter placement should be attempted. However, nephrectomy should be promptly attempted in patients with extensive EPN and signs of organ dysfunction.
Conclusion
Though emphysematous pyelonephritis is rare but in high risk groups such as diabetes presenting with upper urinary tract infection, it should be considered. Emphysematous pyelonephritis with severe sepsis, if recognized and treated early, can decrease the mortality. Prompt diagnosis and early treatment plays an important role in this condition.
References
- Huang JJ, Tseng CC. Emphysematous pyelonephritis: clinicoradiological classification, management, prognosis, and pathogenesis. Archives of Internal Medicine. 2000;160(6):797-805.
-
Shokeir AA, El-Azab M, Mohsen T, El-Diasty T. Emphysematous pyelonephritis: A 15-year experience with 20 cases. Urology. 1997;49(3):343-346.
-
Ubee SS, McGlynn L, Fordham M. Emphysematous pyelonephritis. BJU International. 2011;107(9):1474-1478.
-
Ahlering TE, Boyd SD, Hamilton CL, Bragin SD, Chandrasoma PT, Lieskovsky G, et al. Emphysematous pyelonephritis: a 5-year experience with 13 patients. The Journal of Urology. 1985;134(6):1086-1088.
-
Wang JM, Lim HK, Pang KK. Emphysematous pyelonephritis. Scandinavian Journal of Urology and Nephrology. 2007;41(3):223-229.
-
Tseng CC, Wu JJ, Wang MC, Hor LI, Ko YH, Huang JJ. Host and bacterial virulence factors predisposing to emphysematous pyelonephritis. American Journal of Kidney Diseases. 2005;46(3):432-439.
-
J. Leons SMH, Y. Abu Sara. Emphysematous pyelonephritis: case report. Kuwait Med J. 2004;36(2):134-136.
-
Huang JJ, Chen KW, Ruaan MK. Mixed acid fermentation of glucose as a mechanism of emphysematous urinary tract infection. The Journal of Urology. 1991;146(1):148-151.
-
Tang HJ, Li CM, Yen MY, Chen YS, Wann SR, Lin HH, et al. Clinical characteristics of emphysematous pyelonephritis. Journal of microbiology, immunology, and infection. 2001;34(2):125-130.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Sheikh WR, Mukherjee T, Choudhary SEmphysematous Pyelonephritis.JCR 2015;5:144-146 |
|
Sheikh WR, Mukherjee T, Choudhary SEmphysematous Pyelonephritis.JCR [serial online] 2015[cited 2026 May 27];5:144-146. Available from: http://www.casereports.in/articles/5/1/Emphysematous-Pyelonephritis.html |

|
|
|
|
|