|
|
|
|
|
Gastroschisis in Both Conjoint Twins
|
|
|
G Sudhakar, P Annapurna, R Sasank, K Narasimhulu
Department of Pathology, Siddhartha Medical College, Vijayawada-520008, Andhra Pradesh, India.
|
|
|
|
|
|
Corresponding Author:
|
Dr. G Sudhakar
Email: drgsudhakarjournals@gmail.com |
|
|
|
|
|
|
|
|
Received:
20-JAN-2015 |
Accepted:
10-MAR-2015 |
Published Online:
30-MAR-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Gastroschisis (Greek for “abdominal cleft”) is a full-thickness paraumbilical defect in the abdominal wall. It almost exclusively occurs in infants of mothers younger than 25 years of age. The overall incidence of gastroschisis is 0.94 per 10,000 live births and reports of gastroschisis in both conjoint twins were not available in the literature. It is characterized by normal umbilical cord insertion with defect being extra-abdominal through which abdominal contents protrude. There is no covering sac and the size of the defect is less than 4 cm. This report describes the prenatal diagnosis of a case of conjoint twins complicated with gastroschisis in both the newborns. |
|
|
|
|
|
Keywords :
|
Prenatal diagnosis, Twins, Gastroschisis, Live birth, Infant, Pregnancy.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff3c1f060000009c03000001000700 6go6ckt5b5idvals|445 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Gastroschisis is a rare congenital defect of the anterior abdominal wall that results in the evisceration of abdominal contents. Gastroschisis is a relatively small defect (2 to 4 cm) that involves all layers of the ventral wall. The incidence of gastroschisis is 0.94 per 10,000 live births [1,2,3]. Gastroschisis in both conjoint twins were not reported in literature. The defect is nearly always located just to the right of the umbilicus, although left-sided defects have been described in rare instances [4]. The etiology of gastroschisis is unknown, although several hypotheses have been suggested [5,6].
Case Report
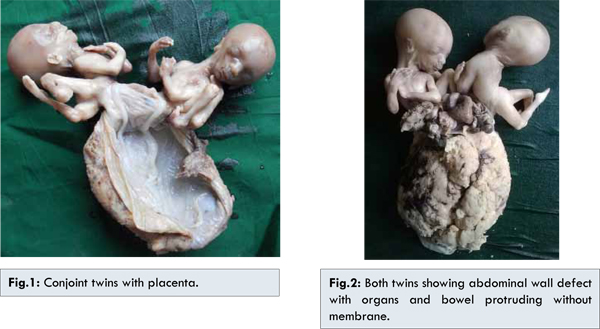
A 27-year-old primiparous female was attended to obstetrics department for regular checkups. Ultrasound at 7 weeks of gestation revealed only single live embryo. But at 16 weeks of gestation it was noted as twin pregnancy with gastroschisis in both twins. There was no family history of abdominal wall defects or any other congenital malformations and no consanguinity. During the pregnancy, the mother denied any medication use, smoking or alcohol consumption but her husband has history of exposure to various petroleum based lubricants and greases. Medical termination of pregnancy was done at 20 weeks of gestation and twins were delivered. Twins with placenta weighed 547 gm and both twins had a 3-cm abdominal wall defect to the right side of the umbilicus with a large portion of the bowel protruding that was uncovered by membrane [Fig.1,2]. There were no other malformations. Gross and histopathological examination revealed the defect of gastroschisis and the attachment of the both twins at the level of the defect.
Gastroschisis has been regarded as a disruption (i.e., an abnormality produced after initial normal development) rather than a malformation (i.e., an abnormality occurring during early embryonic development). However, emerging evidence suggests that gastroschisis may be a malformation. Several hypotheses have been proposed to describe events leading to the development of gastroschisis [5,6]. The incidence of gastroschisis has been increasing worldwide for the past 2 to 3 decades [1,7]. Younger maternal age is consistently reported as a risk factor. The anomaly occurs at four times the baseline rate in women younger than 20 years of age [7].
The general incidence of gastroschisis is 0.94 per 10,000 live births was reported in literature [1,2,3]. There is no statistical data was available in the literature about gastroschisis in both conjoint twins. So we are considering our case as very rare occurrence. Prenatal detection of gastroschisis has been improved by current maternal serum alpha fetoprotein (MSAFP) screening as the defect is associated with an elevation in MSAFP level [8]. There are many conditions that can be associated with an elevated MSAFP, such as neural tube defect, gastroschisis, omphalocele, bilateral renal agenesis and some fetal skin disorders. Ultrasonography is used to differentiate gastroschisis from other conditions that can cause similar serum abnormalities [9]. Gastroschisis has to be differentiated from omphalocele based on the location, size of the defect, presence of sac, type and frequency of anomalies [3,10]. In gastroschisis, the size of the defect is less than 4 cm, extra-umbilical to the right of umbilicus and no overlying sac. Omphalocele itself involves the umbilical cord, the organs remain enclosed in visceral peritoneum and the defect is usually much larger than in gastroschisis [3,11].
Gastroschisis is typically sporadic, although occasional familial cases have been reported, and there has been one report in a pair of monozygotic twins and associated anomalies occur in 5-24% of gastroschisis [11,12]. Hereditary or genetic factors are the most plausible explanation for monozygotic twins with gastroschisis, especially when the mother denies illness or exposure to known teratogenic agents during pregnancy. Further investigation is required to elucidate the role of genetic factors in the etiology of gastroschisis [11].
Conclusion
Gastroschisis in conjoint twins is rare and we could not find any such reported incident on extensive review of literature. So we would like to conclude that this case of gastroschisis in both conjoint twins is a rare occurrence.
References
- Hui-Fen Kao, Hsi-Mi Liang, Chi-Yu Ou, Te-Yao Hsu. Twin pregnancy with gastroschisis in both twins. Taiwan J Obstet Gynecol. 2007;46(4):414-416.
- Martin RW. Screening for fetal abdominal wall defects. Obstet Gynecol Clin North Am. 1998;25:517-526.
- Pei-Jen Hwang, Boris G Kousseff. Omphalocele and gastroschisis: An 18-year review study. Genetics in Medicine. 2004; 6:232-236.
- Suver D1, Lee SL, Shekherdimian S, Kim SS. Left-sided gastroschisis: higher incidence of extraintestinal congenital anomalies. Am J Surg. 2008;195(5):663-666.
- Feldkamp M, Carey J, Sadler T. Development of gastroschisis: review of hypotheses, a novel hypothesis, and implications for research. Am J Med Genet A. 2007;143:639-652.
- Stevenson RE, Rogers RC, Chandler JC, Gauderer MW, Hunter AG. Escape of the yolk sac: a hypothesis to explain the embryogenesis of gastroschisis. Clin Genet. 2009;75:326-333.
- Fillingham A, Rankin J. Prevalence, prenatal diagnosis and survival of gastroschisis. Prenat Diagn. 2008;28:1232-1237.
- Simpson J, Baum L, Marder R, Elias S, Ober C, Martin AO. Maternal serum a-fetoprotein screening: low and high values for detection of genetic abnormalities. Am J Obstet Gynecol. 1986;155:593-597.
- Fillingham A, Rankin J. Prevalence, prenatal diagnosis and survival of gastroschisis. Prenat Diagn. 2008;28:1232-1237.
- Torfs C, Curry C, Roeper P. Gastroschisis. J Paediatr. 1990;116:1-5.
- Mastroiacovo P, Lisi A, Castilla E, Martinez-Frias ML, Bermejo E, Marengo L, et al. Gastroschisis and associated defects: an international study. Am J Med Genet. 2007;143:660-671.
- Torfs CP, Curry CJR. Familial cases of gastroschisis in a population-based registry. Am J Med Genet. 1993;45:465-467.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Sudhakar G, Annapurna P, Sasank R, Narasimhulu KGastroschisis in Both Conjoint Twins.JCR 2015;5:141-143 |
|
Sudhakar G, Annapurna P, Sasank R, Narasimhulu KGastroschisis in Both Conjoint Twins.JCR [serial online] 2015[cited 2026 May 21];5:141-143. Available from: http://www.casereports.in/articles/5/1/Gastroschisis-in-Both-Conjoint-Twins.html |

|
|
|
|
|