|
|
|
|
|
Genital Self-Mutilation: Two Case Reports
|
|
|
RB Nerli, Srikanth P, Ajay Kumar G, Abhijith SM
Department of Urology, KLE University’s J N Medical College, KLES Dr Prabhakar Kore Hospital & MRC, Belgaum, Karnataka, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Ajay Kumar G
Email: drajay707@gmail.com
|
|
|
|
|
|
|
|
|
Received:
22-DEC-2014 |
Accepted:
10-FEB-2015 |
Published Online:
05-MAR-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Psychiatric case reports of male genital self-mutilation (GSM) in the literature are rare and mostly anecdotal. Majority of them are connected with personality disorders. In men, psychosis is an important cause for GSM, causing up to 80% of automutilations. |
|
|
|
|
|
Keywords :
|
Self Mutilation, Scrotum, Psychotic Disorders, Suicide, Personality Disorders, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff8817060000007303000001000d00 6go6ckt5b5idvals|435 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Behaviours that involve damaging the body tissues without intending suicide are defined as self-mutilation [1,2]. Most common types of self-mutilation are damaging the skin, the eyes or the genitals [1]. It is proposed as a fast self-aid action, providing temporary relief from inner tension and confusion [3], depersonalization, feelings of guilt, negative feelings of being rejected, hallucinations and preoccupation with sexual matters [4]. Even if the patient attains temporary relief after the self-mutilation behaviour, pain is said not to be perceived. Although patients suffering from a psychotic disorder, especially schizophrenia, show more tolerance to pain than healthy people, the sense of pain is known not to have completely disappeared [5]. From the beginning of the century to this day, 57 cases of male genital self-mutilation (GSM) have been reported in the English literature. In German publications, we found only five case descriptions. Although no precise data are available on the prevalence of male GSM, such acts are presumably much more frequent than the small number of published cases would suggest. We report 2 patients with personality disorder who had injured their genital organs.
Case Reports
Case 1
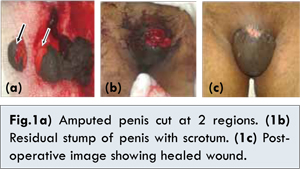
A 38-year-old man was referred to the casualty services, with amputation of penis with razor blade 7 hours back. He was married with no children, and he says his marital relationship as amicable and sexually gratifying. Psychological testing corroborated the absence of psychosis and the likelihood of a primary severe personality disorder. He was cognitively intact and exhibited a normal range of emotions. He credibly denied suicidal inclination. His review of symptoms showed absence of gender-identity disorder features. There was no past or family history of any psychiatric illness, chronic medical illness or drug misuse. He was brought to the hospital in a serious condition. The physical examination revealed an average built patient (weight 59.5 kg, height 165 cm) and an amputed part of penis which was cut into 2 pieces collected in a small bag with superficial laceration (2×5 cm) over the rest of stump of penis and the base of stump tied with a gauze piece for haemostasis [Fig. 1a,b]. As the patient was admitted nearly 7 hours after the injury, no attempt for microsurgical reimplantation was attempted. The penile stump was too small for reconstruction and so decision for perineal urethrostomy was taken. The patient has been under follow-up since 6 months and the wound healed well [Fig. 1c]. He is voiding well from the urethrostomy site.
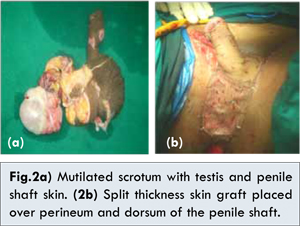
A 45-year-old man was referred to the casualty services, with cutting of the scrotum and testis with laceration of the penile shaft skin over dorsum with a knife 6 hours back. He was married with 2 children. The patient gave no history of previous psychosis or treatment for the same. Psychological testing corroborated the absence of psychosis and the likelihood of a primary severe personality disorder. He was brought to the hospital in a serious condition. The physical examination revealed an average built patient (weight 62 kg, height 160 cm) and an chopped off scrotum with testis in a small bag with superficial laceration (2×5 cm) over dorsum of penis [Fig. 2a]. As the patient was admitted nearly 6 hours after the injury, no attempt for microsurgical reimplantation was attempted. The primary debridement was done with split thickness skin graft over the scrotum wound and on the dorsal surface of shaft of penis [Fig. 2b]. The patient has been under follow-up since 1 month and the graft has taken well.
Genital self-mutilators fall into three groups: psychotics (schizophrenics), transvestites, and patients with complex religious or cultural beliefs. These cases typically involve men. About 110 cases of GSM in men have been described in the literature. In the earlier publications, the majority of these patients were either psychotic or intoxicated during auto-mutilation [6-9]. A review showed that guilt feelings associated with sexual conflicts were the most important factors in the act of psychotic self-mutilation and were also related to religious psychotic experiences that were often the direct motives for the act. Self-mutilators with sexual guilt feelings were likely to mutilate themselves more severely than those without [7]. Suyemoto and MacDonald reported the incidence of self-mutilation in adolescents and young adults between the ages of 15 and 35 to be an estimated 1800 individuals out of 100,000 [10].
The published accounts of genital self-mutilation are almost all either single-case histories or small case series, from which it is difficult to make valid causal inferences. Even quite recent publications sometimes explain genital self-mutilation in terms of the patient’s reaction to passages in religious texts or unconscious sexual conflicts. The few authors who have reviewed more than a small number of cases have attributed genital self-mutilation to the direct effects of psychotic illness [11].
Conclusion
Self-mutilation has been most commonly seen as a diagnostic indicator for borderline personality disorder. Self-mutilating behaviour has been studied in a variety of racial, chronological, ethnic, gender, and socioeconomic populations. People who participate in self-injurious behaviour are usually likeable, intelligent, and functional. At times of high stress, these individuals often report an inability to think, the presence of inexpressible rage, and a sense of powerlessness. In our patients, this aggressive component seems to have been directed against himself, which can mainly be explained by his low self-esteem and insecure personality structure.
References
- Feklman MD. The challenge of self mutilation, a review. Compr Psychiatry. 1988;29: 252-269.
- Dallam SJ. The identification and management of self-mutilating patients in primary care. Nurse Pract. 1997;22:159-165.
- Cavanaugh RM. Self-mutilation as a manifestation of sexual abuse in adolescent girls. J Pediatr Adolesc Gynecol. 2002;15:97-100.
- Favazza AR. The coming age of self-mutilation. J Nerv Ment Dis. 1998;186:259-268.
- Siddiquee RA, Deshpande S. A case of genital self-mutilation in a patient with psychosis. German J Psychiatry. 2007;10:25-28.
- Greilsheimer H, Groves JE. Male genital self-mutilation.Arch Gen Psychiatry. 1979;36:441-446.
- Nakaya M. On background factors of male genital self-mutilation. Psychopathology. 1996;29:242-248.
- Aboseif S, Gomez R, McAninch JW.Genital self-mutilation.J Urol. 1993;150:1143-1146.
- Becker H, Hartmann U. Genital self-inflicted injuries-phenomenological and differential diagnostic considerations from a psychiatric viewpoint. Fortschr Neurol Psychiat. 1997;65:71-78.
- Suyemoto KL,MacDonald ML. Self-cutting in female adolescents. Psychotherapy. 1995;32:162-171.
- Schweitzer I. Genital Self-Amputation and The Klingsor Syndrome. Australian and New Zealand Journal of Psychiatry.1990;24(4):566-569.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Nerli RB, P Srikanth, Kumar G A, SM AbhijithGenital Self-Mutilation: Two Case Reports.JCR 2015;5:100-102 |
|
Nerli RB, P Srikanth, Kumar G A, SM AbhijithGenital Self-Mutilation: Two Case Reports.JCR [serial online] 2015[cited 2026 May 22];5:100-102. Available from: http://www.casereports.in/articles/5/1/Genital-Self-Mutilation.html |

|
|
|
|
|