|
|
|
|
|
Hemopneumothorax Complicating Clavicle Fracture Fixation by K-wire
|
|
|
mixing zoloft and weed mixing viagra and weed read
From the Departments of Emergency Medicine1 and Thoracic Surgery2; Dicle University, Diyarbakir, Turkey. |
|
|
|
|
|
Corresponding Author:
|
Dr. Recep Dursun
Email: drrecepdursun@hotmail.com
|
|
|
|
|
|
|
|
|
Received:
25-NOV-2014 |
Accepted:
6-FEB-2015 |
Published Online:
25-FEB-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Clavicle fractures are largely treated by conservative methods, but there are numerous fractures requiring surgery. In our case, clavicle fracture had occurred approximately 6 month earlier secondary to the trauma and had been fixed by Kirschner wire (K-Wire). The case presented with hemopneumothorax. Tube thoracostomy was done and K-wire removed. Current surgical options like K-wire for clavicle fractures may be associated with unacceptable complications, and less invasive approaches may be adopted. |
|
|
|
|
|
Keywords :
|
Hemopneumothorax, Clavicle, Bone Wires, Fractures, Pseudoarthrosis, Thoracostomy, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff7c17060000007c03000001000300 6go6ckt5b5idvals|432 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Clavicle fractures constitute 4-12% of all fractures and also approximately 35-40% of fractures related to shoulder belt. [1]. Clavicle is one of the bones which fractures frequently owing to its anatomic location and biomechanical characteristics. Although clavicle fractures are seen frequently, bonding problems are scarce [2]. Pseudoarthrosis rate in clavicle ranges between 0.1-0.5% [3]. Complications following clavicle fixation surgery may be overlooked, therefore surgical treatment must be avoided [2, 3].
Case Report
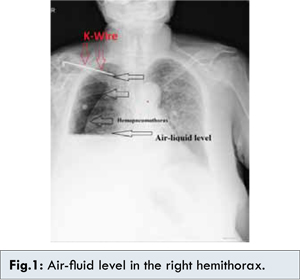
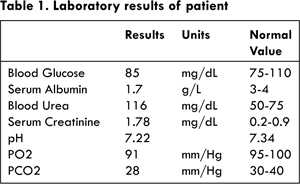
A case of right clavicular fracture fixed with Kirschner wire (K-wire) six months earlier presented with shoulder pain, deformation in the right clavicle region and respiratory difficulty. On physical examination, there was right shoulder deformity and lung sounds were not perceived in right hemithorax with tympanic sound in the upper and middle zones on percussion and dullness in the lower zone. Chest radiograph revealed distal end of K-wire to be separated from right clavicle with hydro pneumothorax giving air-liquid level in the right hemithorax [Fig.1]. There were hypotension, tachycardia and tachypnea in patient. Laboratory results as shown in Table 1 were suggestive of acidosis, hypoalbuminemia and elevated urea and creatinine values.
Thoracocentesis was done at mid-axillary intercostal space and hemorrhagic fluid was drained. 32 F size tube thoracostomy was placed to the same side. Approximately 2000 ml of accumulated hemorrhagic fluid was drained subsequently. K-wire was removed and conservative approach was adopted instead of additional surgical treatment. Supportive measures were taken to correct metabolic disturbance however the general as well as respiratory condition of the patient worsened and he had to be shifted to intensive care unit under clinical suspicion of acute respiratory distress syndrome [Fig.2] where he was intubated. Despite all treatment and supportive measures the patient expired.
Discussion
Clavicle fractures are encountered frequently but joining problems are rare [2]. Although significant level of recovery is achieved by the open reduction and internal fixation of clavicle fractures, in the treatment of these fractures, majority of orthopedic surgeons adopt a conservative approach. However, it is not very realistic assumption that the entirety of these fractures will bond appropriately by the conservative treatment [4]. According to Manske, surgical indication follows an unsuccessful conservative treatment in clavicle fractures [5]. It is observed that segmental and problematic fractures may have earlier surgical indication [2]. There is no consensus on the surgical method of choice for treatment of clavicle fractures. In practice various methods are used such as cerclage with wire, osteosynthesis with K-wires, osteosynthesis with McKeever screws, and osteosynthesis with plates [5]. It is known that of many implants used in internal fixation, K-wire mostly leads to transposition.
Although transposition takes place in retrograde direction, if it happens in anterograde direction, serious complications may occur. In our case, it was seen that K-wire slipped towards the distal mediastinum (superior vena cava). Since we presumed that this situation would be dangerous if wire was not removed. It is possible to see cases that K-wire transposed toward lungs, heart, subclavian artery, pulmonary artery, and aorta [6]. There are cases notified about such type of movement. Potter et al. [7] reported that K-wire transposed from the shoulder region towards the spleen, and Fuster et al. [8] reported that it transposed from the shoulder to the opposite hemithorax. Moreover, they also reported about cases harming major vascular structures. Salvatore et al. [9] reported about transposition to the heart, Grauthoff et al. [10] reported about transposition to subclavian artery, and Janssens et al. [11] reported about transposition to pulmonary artery. Cases with death were also reported due to transposition of K-wire [6]. The reason for transposition was accounted for the movement of surrounding muscles, gravity, and capillary action. However the primary reason is not known [7]. It is necessary that the patients are selected well for K-wire application for avoiding such complications and they must be called for frequent follow ups.
Conclusion
Irrespective of type of wire used in bone injuries a close follow up is necessary to monitor for possible injury to neighboring vital organs. Patients should be made aware of possible complications and emphasis should be made on regular follow up and recognition of early signs of complications.
References
- Van Der Meijden OA, Gaskill TR, Millett PJ. Treatment of clavicle fractures: current concepts review. J Shoulder Elbow Surg. 2012;21(3):423-429.
- Galvin JW, Dannenbaum JH, Grassbaugh JA, Eichinger JK. Pseudarthrosis of the clavicle. Orthopedics. 2014;37(5):295, 349-350.
- Wilkins RM, Johnston RM. Ununited fractures of the clavicle. J Bone Joint Surg Am. 1983;65(6):773-778.
- Zenni EJ, Krieg JK, Rosen MJ. Open reduction and internal fixation of clavicular fractures. J Bone Joint Surg Am. 1981;63(1):147-151.
- Manske OJ, Szabo RM. The operative treatment of mid-shaft clavicular non-unions. J Bone Joint Surg Am. 1985;67(9):1367-1371.
- Bezer M, Aydin N, Erol B, Laçin T, Güven O. Unusual migration of K-wire following fixation of clavicle fracture: a case report: a casereport: Ulus Travma Acil Cerrahi Derg. 2009;15(3):298-300.
- Potter FA, Fiorini AJ, Knox J, Rajesh PB. The migration of a Kirschner wire from shoulder to spleen: brief report. J Bone Joint Surg Br. 1988;70(2):326-327.
- Fuster S, Palliso F, Combalia A, Sanjuan A, Garcia S. Intra thoracic migration of a Kirschner wire. Injury. 1990;21(2):124-126.
- Salvatore JE. Sterno clavicular joint dislocation. Clin Orthop Relat Res. 1968;58:51-55.
- Grauthoff H, Klammer HL. Complications due to migration of a Kirschner wire from the clavicle (author’s transl). Rofo. 1978;128(5):591-594.
- Janssens de Varebeke B, Van Osselaer G. Migration of Kirschner’s pin from the right sternoclavicular joint resulting in perforation of the pulmonary artery main trunk. Acta Chir Belg. 1993;93(6):287-291.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Dursun R, Oruç M, Öztürk B, Onat SHemopneumothorax Complicating Clavicle Fracture Fixation by K-wire.JCR 2015;5:88-90 |
|
Dursun R, Oruç M, Öztürk B, Onat SHemopneumothorax Complicating Clavicle Fracture Fixation by K-wire.JCR [serial online] 2015[cited 2026 May 27];5:88-90. Available from: http://www.casereports.in/articles/5/1/Hemopneumothorax-Complicating-Clavicle-Fracture-Fixation-by-K-wire.html |

|
|
|
|
|