Introduction
The spleen is one of the most commonly injured intra-abdominal organs in blunt trauma. While every attempt is made to save the spleen when involved, emergent and urgent splenectomy remains a life-saving measure in case of ongoing hemorrhage. The surgical options for splenic injury whenever indicated have been either a complete splenectomy or in certain cases lesser procedures like partial splenectomy or more conservative measures like splenorrhaphy and hemostatic collagen application. Till recent, these procedures have been done in an open fashion through an exploratory laparotomy. Laparoscopic splenectomy though first described in literature by Delaitre and Maignien in 1991 [
1], has mostly been used in an elective setting. With technologic advances and improved laparoscopic instrumentation, it has become possible to manage blunt trauma cases laparoscopically.
A few isolated case reports exist in the literature of laparoscopic splenectomy following blunt trauma. Basso et al. from Italy in 2003 reported laparoscopic splenectomy 10 days post injury for a grade IV ruptured spleen [
2]. Nasr et al. from United States in 2004 reported a series of 4 stable patients undergoing delayed laparoscopic splenectomy for blunt trauma [
3]. The largest published experience is by Huscher et al. who reported laparoscopic treatment of 11 cases for blunt splenic injuries [
4]. We present a case of successful treatment of a high grade splenic injury from blunt trauma in a young stable person, using a total laparoscopic approach, which to our best knowledge, has rarely been reported.
Case Report
A 15 year old boy presented to the ER of our hospital with abdominal pain, after a fall from a 2-wheeler in a road traffic accident. At presentation he was conscious, oriented and hemodynamically stable. On abdominal examination, he had tenderness and guarding on the left side of the abdomen, with a relatively soft right side. There was no rebound tenderness. Additionally, he had a lacerated wound over his left iliac crest, with local tenderness. Contrast CT abdomen and chest revealed grade IV splenic injury [Fig.1,2] with associated hematoma, hemoperitoneum, fracture left 7th, 8th & 9th ribs, and left lower lobe lung contusions. CT pelvis showed comminuted fracture of the left iliac crest. A trial of conservative management was given to begin with. His hemoglobin level at presentation was 13.9 g/dL, but it continued to fall sharply over a period of 2 hours to 11.6 g/dL and then to 10.3 g/dL in the next hour. His heart rate increased to 116/min, and BP 108/60 mmHg. With the absence of the option of embolization at our facility, the treatment options of continued non-operative management, or emergency splenectomy were discussed with the patient’s family, understanding the risks-benefits of each modality. A decision of laparoscopic, possible open splenectomy was taken after informed consent from the father.
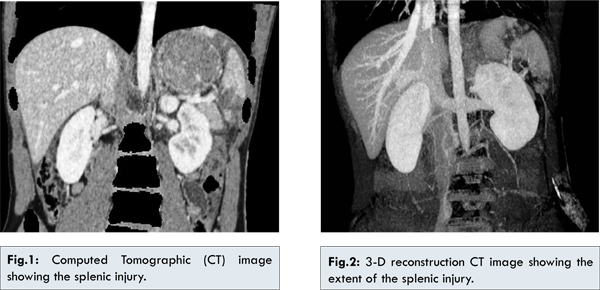
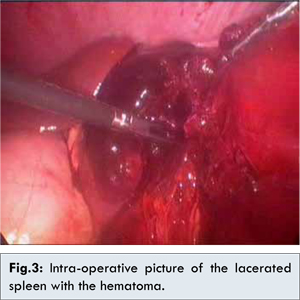
After inducing general anesthesia, the patient was put in a 45° modified right lateral position. Body and arms were adequately padded and strapped. The stomach was sucked out by an oro-gastric tube. After usual prepping and draping, pneumoperitoneum was achieved with a Veress needle via a left subcostal approach. A 10 mm camera port was put at the linea semilunaris at the level of the umbilicus using an optical viewing trocar (Endopath Xcel, Ethicon Endo-Surgery, Cincinnati, OH). Two more 5 mm ports were then put under direct vision, one below the xiphoid process and other left subcostal in the anterior axillary line. A 12 mm port for the stapler was put left subcostal in the posterior axillary line. A 10 mm 30° laparoscope was then introduced and a diagnostic laparoscopy performed. A large splenic hematoma was noted [Fig.3] along with approximately 1.5 liters of hemoperitoneum, which was sucked out. No other injury in the abdomen was seen. The dissection was commenced by taking down the splenic flexure of colon, followed by the lateral attachments of the spleen, taking down the highest diaphragmatic attachments. The lesser sac was then entered anteriorly, and the short gastrics taken down till the gastric cardia was totally freed of its attachment with the spleen. The spleen was seen to be nearly broken into three pieces with two lacerations, one towards the upper pole, and other towards the lower pole, with a cyanosed middle segment, which corresponded with the pre-operative CT picture [Fig.2]. Hilar dissection was then commenced, carefully separating and preserving the tail of the pancreas. The splenic vascular pedicle was then divided with a linear stapler (Echelon 60, Ethicon Endosurgery, Cincinnati, OH). Hemostasis was checked at the staple line. An indigenously made specimen retrieval plastic bag was then introduced into the peritoneal cavity and the spleen put into the bag. A ring forceps was then used to fracture the spleen in the bag and remove it in a piece-meal fashion. The bag was pulled out of the 12 mm port site. Thorough peritoneal toilet was then done, and hemostasis checked again at the staple line. A 14 No. closed suction drain was put in the splenic bed area. The 12 mm port site fascia was closed. The total operating time was 135 minutes. Patient tolerated the procedure well. He was relatively pain free from post-operative day (POD) # 1, ranging 1-2/10 on the pain scale. From POD # 2 onwards he did not report any pain, a 0-1/10, and was off scheduled pain medication, to be given oral analgesics on an ‘as needed’ basis only. His hemoglobin level stabilized between 11.5-12.0 g/dL before discharge. The abdominal drain was taken out on POD # 2. The left iliac wound was managed conservatively by the orthopedic team, and the patient was able to walk with the help of a walker by the day of the discharge. He was discharged on POD # 4. Pneumococcal, Meningococcal and H. Influenza vaccines were administered before discharge.
The incidence of splenic injury in blunt abdominal trauma has been reported as high as 25% in literature [
5]. The management has undergone major changes over the past from nearly mandatory laparotomy with splenectomy, to an increase in non-operative management with every effort made to preserve the spleen, and of recent the use of minimally invasive surgery. But broadly, the generalized consensus is that the hemodynamically unstable patients bleeding from splenic injury must be taken immediately to the operating room for urgent laparotomy and splenectomy or splenorrhaphy. Patients who are more stable should be evaluated for non-operative management.
Close observation has become an accepted treatment of stable splenic injuries from blunt trauma [
6], with a variable failure rate ranging from 10% to 40% [
7]. High grade splenic injuries (grade III and higher) tend to have a higher failure rate, along with a higher transfusion requirement and increased morbidity and mortality [
8]. Further risks of non-operative treatment include delayed splenic rupture, persistent pain, and prolonged immobilization which are contraindicated in a group at high risk for venous thromboembolism. The need for bed rest and monitoring often requires prolonged hospital stays. One of the main reasons for advocating splenic preservation is the possibility of an overwhelming post-splenectomy sepsis (OPSI). However, the incidence of OPSI in adults, in contrast with children, is very low (<1%) and with modern vaccination and antibiotics is expected to decline further. In adult patients, the risks of transfusion and delayed splenic rupture, abscess, and pain should be weighed against the risk of OPSI in determining the best approach to severe splenic injuries.
Splenic artery angio-embolization has been described as an alternative to operative management of splenic injuries. Smith et al. in 2006 reported that even though embolization significantly decreases the need for splenectomy, 5% to 20% of patients have been reported to continue bleeding following embolization [
9]. He reported that embolization was associated with a non-operative failure following high grade injury (III at 40%, IV at 38%, and V at 40%), moderate to large associated hemoperitoneum (36%), and extravasation at the time of angiography (59%). When extravasation was associated with a moderate to large hemoperitoneum, the failure rate was 71%. Complications of angio-embolization include the need for delayed splenectomy due to splenic infarction, infection, abscess or persistent pain [
10,
11]. In those institutions where a vascular surgeon or radiology specialist for embolization is available 24 hours a day, this could be a preferred option. But, when such a facility is not available, and conservative management is doubtful otherwise, splenectomy may be the best option, particularly if the splenectomy can be performed laparoscopically.
The role of laparoscopy in blunt trauma has yet to be clearly defined, yet laparoscopic exploration in trauma has been attempted and cited as an acceptable option in literature [
12-
15]. Trauma laparoscopy has been reported as a safe method for the evaluation of selected patients with abdominal trauma, which could reduce the number of negative and non-therapeutic trauma laparotomies performed [12,16]. Several authors have used laparoscopy to apply hemostatic agents to solid organ lacerations and perform spleen preserving procedures in lower grade injury [
13,
14]. The risk of injury to the tail of the pancreas during a laparoscopic dissection of the splenic hilum in the presence of a hematoma/ hemoperitoneum is not different from an exploratory laparotomy in experienced hands. We believe that with the laparoscopic technique, the experience of the surgeon and the visualization of the hilum are of utmost importance, and the pancreatic tail can be visualized well and decrease the risk of the pancreatic tail injury. Apart from affording the usual benefits of minimal invasive surgery, it also tends to have decreased intra-operative blood loss and transfusion requirements.
We are reporting this case in support of the existing literature that laparoscopic splenectomy may potentially be the treatment of choice in hemodynamically stable patients, with a CT documented isolated splenic injury. The question remains though, who should attempt laparoscopic splenectomy and who should not, which would largely depend on the experience of the surgeon and the comfort level with the laparoscopic technique in such cases. Our patient was able to resume a regular diet from the next day and had minimal requirements for pain medication. The reason he stayed in the hospital for 4 days was mainly to recoup from his pelvic injury, otherwise a patient with an isolated splenic injury may likely be stable enough to be discharged the next day, following laparoscopic surgery.
In conclusion, this case, along with the other limited reports in the literature, suggests laparoscopy could be a safe, feasible, and effective modality of evaluation and treatment of hemodynamically stable patients with high grade splenic injuries.
References
- Delaitre B, Maignien B. Laparoscopic Splenectomy - technical aspects. Surg. Endosc. 1992; 6:305.
- Basso N, Silecchia G, Raparelli L, Pizzuto G, Picconi T. Laparoscopic splenectomy for ruptured spleen: lessons learned from a case. J Laparoendoscopic Adv Surg Tech A. 2003;13(2):109-112.
- Nasr WI, Collins CL, Kelly JJ. Feasibility of laparoscopic splenectomy in stable blunt trauma: a case series. J Trauma. 2004;57:887-889.
- Huscher CGS, Mingoli A, Sgarzini G. Laparoscopic treatment of blunt splenic injuries: initial experience with 11 patients. Surg Endosc. 2006;20:1423-1426.
- David B. Hoyt, Raul Coimbra, Sandra Engelhardt. Trauma - Specific injuries; Essential Surgical Practice. 4th Ed. 2002;1:17.
- Haan JM, Bochicchio GV, Kramer N, Scalea TM. Nonoperative management of blunt splenic injury: a 5 year experience. J Trauma. 2005;58(3):492-498.
- Knudson MM, Maull KI. Nonoperative management of solid organ injuries. Surg Clin North Am. 1999;79:1357-1371.
- Jalovec LM, Boe BS, Wyffels PL. The advantages of early operation with splenorrhaphy versus nonoperative management for the blunt splenic trauma patient. Am Surg. 1993;59:698-705.
- Smith HE, Biffl WL, Majercik SD. Splenic artery embolization: have we gone too far? J Trauma. 2006;61:541-546.
- Dissanaike S, Frezza EE. Laparoscopic splenectomy in blunt trauma. JSLS. 2006;10:499-503.
- Huscher CG, Mingoli A, Sgarzini G, Brachini G, Ponzano C, Di Paola M. Laparoscopic treatment of blunt splenic injuries: Initial experience with 11 patients. Surg Endosc. 2006;20:1423-1426.
- Chol YB, Lim KS. Therapeutic laparoscopy for abdominal trauma. Surg Endosc. 2003;17(3):421-427.
- Shen HB, Lu XM, Zheng QC, Cai XT, Zhou H, Fei KL. Clinical application of laparoscopic spleen-preserving operation in traumatic spleen rupture. Chin J Traumatol. 2005;8(5):293-296.
- Orcalli F, Elio A, Veronese E, Frigo F, Salvato S, Residori C. Conservative laparoscopy in the treatment of posttraumatic splenic laceration using microfiber hemostatic collagen. Surg Laparosc Endosc. 1998;12:600-603.
- Simon R, Rabin J, Kuhls D. Impact of increased use of laparoscopy on negative laparotomy rates after penetrating trauma. J Trauma. 2002;53:297-302.
- Smith RS, Fry WR, Morabito DJ. Therapeutic laparoscopy in trauma. Am J Surg. 1995;170(6):632-637.