Introduction
Gastroschisis is a defect of anterior abdominal wall, which means belly cleft in Greek [
1]. Gastroschisis is an uncommon ventral body wall defect with continuing challenge to researchers, clinicians and epidemiologists. It is herniation of abdominal contents through paramedian full thickness abdominal wall defect without involving the umbilical cord [
2]. Incidence is 1 in 20,000 births, which is reportedly increasing [
3]. Associated risk factors include young maternal age, low parity, low birth weight and growth retardation [
4]. We report an aborted fetus with left sided gastroschisis with liver agenesis, rudimentary left lung and left pulmonary artery.
Case Report
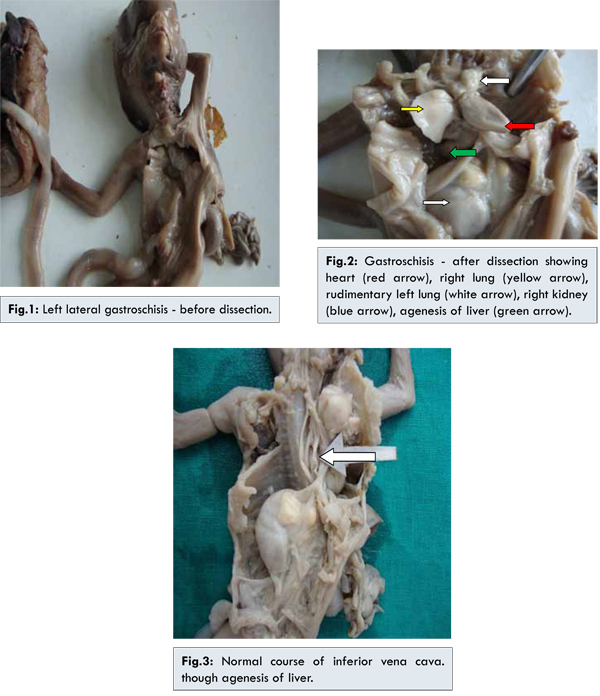
We received 18 weeks aborted fetus from obstetrics department. Mother was 20 year old second gravida. The pregnancy history was negative for significant complications like diabetes, hypertension, teratogenic exposures or family history of congenital abnormalities. First pregnancy was uneventful and had normal female child of 2 years age. She was an unbooked case with no previous antenatal visits or investigations like ultrasound. Fetus weighed seven hundred grams, had multiple congenital anomalies with left side abdominal wall defect of four centimeters in diameter. Abdominal contents eventuated from the defect and were not covered by membranes. Most of the large and small intestines matted together with respective blood vessels and left kidney was herniated out [Fig.1]. Postmortem examination revealed gastrochisis to left of abdomen 4 cm in diameter. No membranes covering the organ were seen. Right kidney was in normal position and both ureters were opening into bladder. Left lung and left pulmonary artery were rudimentary. Right lung and right pulmonary artery were normal. Liver was absent [Fig.2]. Course of inferior vena cava was normal, opening into inferior aspect of right atrium, though agenesis of liver [Fig.3]. Abdominal aorta course was normal. Genital organs were well developed.
In the spectrum of abdominal wall defects, gastroschisis and omphaloceleare are most common and they generally occur between the 4 to 9 weeks of gestation [
5]. Other names to describe gastroschisis include paraomphocoele, laproschisis and abdomioschisis [
2]. Four main hypotheses proposed in the pathogenesis of gastroschisis include (i) failure of mesoderm to form body wall. (ii) rupture of amnion around umbilical ring. (iii) abnormal involution of right umbilical vein leading to weakening of body wall and gut herniation. (iv) disruption of right vitalline artery with subsequent body wall damage and gut herniation [
4]. Recreational drugs like aspirin, tobacco, cocaine and amphetamine increase the risk. Gastroschisis occurs more frequently in mothers who are exposed to agricultural chemical atrazine [
6]. Gastroschisis is not associated with chromosomal anomalies and is a sporadic malformation [
7].
The defect is almost right lateral to the umbilicus and not covered by membranes. Left sided gastroschisis is extremely rare [
8]. In our case left paraumbilical gastroschisis was observed. Usually non-rotated small bowel eviscerates through the defect lacking secondary fixation to posterior abdominal wall. The intestines directly exposed to amniotic fluid are matted together, hence alpha-fetoprotein levels are high. In 25% of cases gastrointestinal problems are associated [
7]. Partial agenesis of liver have been reported with reported incidence of right lobe agenesis common than the left lobe [9]. We observed complete agenesis of liver and normal course of inferior vena cava, which was not reported in the literature. Pankaj Prasun et al. reported left gastroschisis with herniation of left polycystic kidney [
8]. We observed herniation of normal left kidney. Gastroschisis without herniation of major viscus has better prognosis than omphalocele. In our case, hypoplastic left lung was observed as reported by Hebbar et al [
2]. According to literature agenesis of left lung is common than right lung [
10]. Prune belly syndrome is well preserved, poor abdominal wall formation associated with urinary tract and intestinal malformations [
6], but in this case no urinary or intestinal malformations were observed.
Conclusion
Gastroschisis has good prognosis, but in our case intrauterine death of the fetus may be due to multiple congenital anomalies like hypoplastic left lung and complete liver agenesis.
References
- Ravi PR, Gupta A. Management of Gastroschisis in a Remote Hospital. MJAFI 2008; 64:175-176.
- Hebbar, Shripad N, Kumar P. An unusual case of foetal gastroschisis with limb aplasia and extra-corporal liver. Calicut Medical Journal. 2005;3(3).
- Zamakhshary M, Yanchar NL. Complicated gastroschisis and maternal smoking: a causal association? Pediatric Surgery International. 2007;23(9):841-844.
- Stevenson RE, Rogers RC, Chandler JC, Gauderer MW, Hunter AG. Escape of the yolk sac: a hypothesis to explain the embryogenesis of gastroschisis. Clin Genet. 2009;75(4):326-333.
- Stepan H, Horn LC, Bennek J, Faber R. Congenital hernia of the abdominal wall: a differential diagnosis of fetal abdominal wall defects. Ultrasound Obstet Gynecol. 1999;13:207-209.
- Sunitha V. The Macroscopic & Microscopic Study of Associated Variant Viscera in a Gastroschisis Foetus. International Journal of Health Sciences & Research. 2012; 82(1):82-89.
- Fernando Bonilla-Musoles, Luiz Eduardo Machado, Luiz Antonio Bailao, Newton G. Osborne, Francisco Raga. Abdominal Wall Defects. Two-Versus Three-dimensional Ultrasonographic Diagnosis. J Ultrasound Med. 2001;20:379-389.
- Prasun P, Pradhan M, Kumari N, Das V. Left- sided gastroschisis and bilateral multicystic dysplastic kidneys: a rare combination of anomalies. Prenatal Diagnosis. 2007;27:872-873.
- Yan Ling Wen, Masatoshi Kudo SJSUM, Hobyung Chung, Yasunori Minami, Youichiro Suetomi, Hirokaza Onda, et al. Agenesis of the left lobe of the liver: Radiological findings. Journal of Medical Ultrasonics. 2001;28(4):181-183.
- Dutta D, Karlekar A, Saxena R. Agenesis of the lung. Annals of Cardiac Anaesthesia. 2013;16(2):151-152.