Introduction
Multicentric reticulohistiocytosis (MRH) is a rare disease with frequent involvement of bones, tendons, muscles and joints. Females are affected more than men, with the ratio of woman to man being 3:1 [
1]. Skin involvement generally establishes with translucent reddish-brown to flesh-colored papulonodules varying from 1-2 mm to 1 cm in diameter or larger. In MRH, papulonodular skin lesions are often associated with arthritis [
2].
Case Report
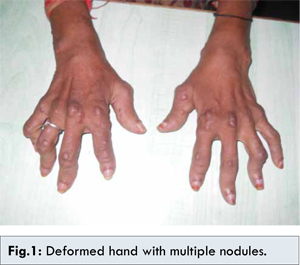
A 32 years old female presented with arthritis involving the small joints of the both hands and feet with minimal morning stiffness since last 6 months. It progressed rapidly, involving distal inter-phalangeal joints of the hand, wrist and elbow. Lower limb joints were minimally involved. She had painless multiple nodules (0.5-1.0 cm) over the extensor aspect of the hand and forearm [Fig.1] prior to the onset of arthritis. This was associated with swelling and deformity of the joints. Her history was not suggestive of weight loss, loss of appetite, fever, chronic cough and consumption of methotrexate.
Her ESR was 20 mm/hour, CRP 12 mg/dL, with negative rheumatoid factor, negative cyclic citrullinated peptide, negative antinuclear antibody and normal serum creatinine. X ray for both the hands showed erosions in the head of proximal and intermediate phalanx with periarticular swelling with normal carpal bones, and distal interphalangeal joint having erosion of proximal end plate of distil phalanx [Fig.2]. Her chest X ray and ultrasound abdomen were normal. Biopsy of the nodule showed subepithelial aggregates of histocytes and giant cells suggestive of reticulohistiocytosis [Fig.3].
Discussion
Rapidly progressive erosive arthritis can be seen in rheumatoid arthritis, psoriatic arthritis (arthritis mutilans), pseudo rheumatoid presentation of gout and in MRH. Rheumatoid arthritis patients when on treatment with methotrexate can develop nodulosis. Chronic tophaceous gout also can have multiple nodules with erosive arthritis. This patient had arthritis mutilans with distal interphalangeal (DIP) joint involvement and papulonodular lesions with aggregate of histocytes and giant cells suggestive of MRH.
MRH is a rare condition with approximately 200 cases reported in the world literature. Various diseases have been associated with MRH, including malignancy [
3]. The pathogenesis of MRH is unknown but probably has an immunologic basis. Some studies have demonstrated increased levels of tumor necrosis factor (TNF) a in the blood and in the tissue [
4]. The primary manifestations of MRH are joint and skin diseases. Inflammatory joint disease is a frequent presenting symptom, and it is the sole symptom in 45% of patients. Skin disease is common, and it is the presenting manifestation in 30% of patients. Biopsy of the skin nodule showed histocytes and multinucleated giant cells, with a pale, fine, granular (i.e. ground-glass) eosinophilic cytoplasm filling the dermis. Synovial biopsy was similar as skin and may be useful in diagnosing rapidly progressive arthritis without skin nodules.
Nonspecific pulmonary findings, such as pleural effusions and infiltrates, have been reported in association with MRH [
5]. Follow up of patient is essential as malignancies associated with MRH include melanoma, sarcoma, leukemia, lymphoma, bladder and renal cancer, squamous cell carcinoma of the lung, liver carcinoma, and carcinomas (usually adenocarcinoma) of the breast, colon, bronchus, cervix, stomach, and ovaries [
6]. Radiography of the affected joints reveals destruction of bone disproportionate to loss of cartilage. Lesions may resemble gouty erosions. Mild osteopenia is noted. Marked resorption of subchondral bone is common. The findings may develop rapidly and can resemble arthritis mutilans. It is less useful in differentiating from other rapidly progressive arthritis. No effective treatment is available. NSAIDS, methotrexate, antimalarial, cytotoxic drugs like cyclosporine, cyclophosphamide may be effective. Recently TNF alpha inhibitor with methotrexate has shown to be effective [
4]. This patient is currently on methotrexate of 15 mg/week with a good response.
Conclusion
Effective management of MRH requires prompt suspicion, synovial biopsy in cases presenting with arthritis as sole presentation, appropriate therapy and regular follow up to rule out malignancy.
References
- Sroa N, Zirwas MJ, Bechtel M. Multicentric reticulohistiocytosis: A case report and review of the literature. Cutis. 2010;85(3):153-155.
- Shah SP, Shah AM, Prajapati SM, Bilimoria FE. Multicentric reticulohistiocytosis. Indian Dermatol Online J. 2011;2(2):85-87.
- Nunnink JC, Krusinski PA, Yates JW. Multicentric reticulohistiocytosis and cancer: a case report and review of the literature. Med Pediatr Oncol. 1985;13(5):273-279.
- Kovach BT, Calamia KT, Walsh JS, Ginsburg WW. Treatment of multicentric reticulohistiocytosis with etanercept. Arch Dermatol. 2004;140(8):919-921.
- West KL, Sporn T, Puri PK. Multicentric reticulohistiocytosis: a unique case with pulmonary fibrosis. Arch Dermatol. 2012;148(2):228-232.
- Tan BH, Barry CI, Wick MR. Multicentric reticulohistiocytosis and urologic carcinomas: a possible paraneoplastic association. J Cutan Pathol. 2011;38(1):43-48.