Introduction
Jejunal diverticula are the rarest of all small bowel diverticula with an incidence of 0.1-1.5% [1]. They are pseudodiverticula resulting from increased intraluminal pressure along with bowel wall weakening. The majority of patients with jejunal diverticula are asymptomatic, discovered incidentally on radiological investigation. Chronic abdominal symptoms like abdominal pain, nausea, flatulence, diarrhea and malabsorption have been attributed to them. Jejunal diverticulosis may present acutely with complications in 10-30% of all patients [2,3]. These include diverticulitis, abscess formation, intestinal obstruction, hemorrhage or diverticular perforation. Complicated presentations remain a diagnostic challenge because of varied and nonspecific symptoms. Surgery is indicated as the treatment of choice for almost all acute complicated cases. We present a rare case of acute abdomen caused due to a perforated jejunal diverticulum. We also review the literature associated with the management of small bowel diverticular perforation.
Case Report
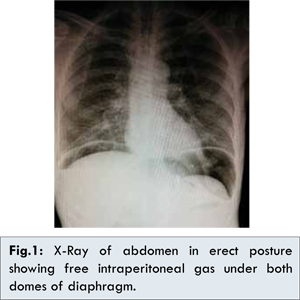
A 76 year old male presented to the emergency department with a three day history of generalized abdominal pain with few episodes of vomiting. Past medical history was significant for ischemic heart disease and hypertension. He was febrile, tachycardic (pulse:110 beats/min) and hypotensive (blood pressure: 90/60 mm Hg). On examination, he had signs of peritonitis with generalized muscle guarding and severe tenderness in epigastric and periumbilical region. Bowel sounds were absent. Laboratory investigations revealed deranged renal function (serum urea: 67 mg/dL, serum creatinine: 2.2 mg/dL) and elevated leucocyte count (17000 cells/mm3) with left shift. X-ray of abdomen in erect position showed few dilated loops of small bowel with intra-peritoneal free air under both domes of diaphragm [Fig.1]. A diagnosis of perforation peritonitis was made.
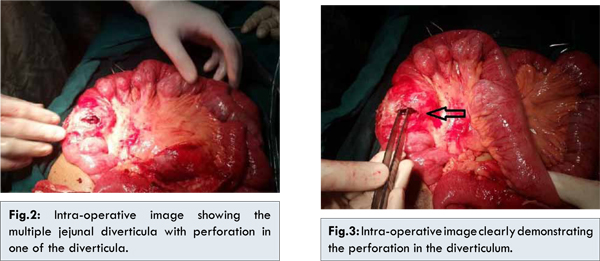
The patient was resuscitated with intravenous fluids and antibiotics. Emergency surgery was planned and the patient underwent a laparotomy by midline incision. Intra-operatively, there were multiple jejunal diverticula at mesenteric aspect of the jejunum between 30 cm and 80 cm from duodeno-jejunal flexure of Treitz. There was evidence of diverticulitis with a single large perforation in one of the diverticula with associated peritoneal contamination [Fig.2,3]. The entire diverticulum bearing segment of jejunum was resected [Fig.4] and end to end jejuno-jejunal anastomosis was performed. Thorough peritoneal washout was performed. Postoperatively, the patient had superficial surgical site infection, which resolved with local wound care and antibiotics. The patient made a good recovery, and was discharged on 9th postoperative day.

Histopathological examination revealed the diverticulae to be composed of mucosa and submucosa only i.e. they were pseudo-diverticulae. The perforated diverticulum showed necrosis with acute inflammatory infiltrate and fibrinous exudate.
Discussion
Jejunal diverticula as an entity was first described in 1794 by Somerling and by Sir Astley Cooper in 1807 [4]. They are pseudo-diverticulae in that they are composed only of mucosa and submucosa which herniate through the gaps in the muscle layers along the path of blood vessels on the mesenteric aspect of bowel wall. The etiology is unclear; however it is believed to develop from a combination of abnormal peristalsis, intestinal dyskinesia and high segmental intra-luminal pressures [5]. They are generally multiple and vary in size from few millimeters to more than ten centimeters. They are more common in the elderly and have slight male preponderance [1]. The exact incidence is difficult to ascertain but estimated to be around 2.0–2.3% on enteroclysis and on autopsy it is 0.06-4.6% [5,6]. Jejunal diverticula may be the only site in the gastrointestinal tract or it may be coexistent with diverticula at other sites. In patients with jejunal diverticula, 35% have associated colonic diverticula, 26% have duodenal diverticula and 2% have oesophageal diverticula [7,8].
Clinical presentation of jejunal diverticula is highly variable [1,5]. Diagnosis may be missed or delayed due to the rarity of the condition and failure to maintain a high index of suspicion. The condition remains asymptomatic in over 80% of affected individuals [5]. It may present with chronic clinical manifestations which include vague abdominal discomfort, fullness, recurrent abdominal cramping pain caused by pseudo-obstruction or bacterial overgrowth [7]. The chronic symptoms combined with normal radiological investigations may lead to an erroneous diagnosis as irritable bowel syndrome or dyspepsia. However, confirmation of diverticulosis as the source of these symptoms is only possible with cessation of the symptoms with resection of affected part of the bowel.
Complications associated with small bowel diverticular disease are rare. 10-30% of affected individuals present with complications like obstruction, perforation or hemorrhage [2]. Perforation is rare, occurring in less than 6% of all patients with diverticula [9]. This may be related to the low intraluminal pressures within the small bowel. Causative factors for perforation been shown to be due to necrotizing inflammatory reaction in 82%, blunt trauma in 12% of cases and foreign body impaction in 6% of cases [10]. Diverticular inflammation and perforation usually leads to abscess formation in the mesentery of the small bowel. Generalized peritonitis is uncommon because the mesenteric location of the diverticula allows them to be walled off effectively.
Jejunal diverticulosis poses a diagnostic challenge, because none of the radiological investigations are truly reliable. Abdominal radiographs may be diagnostic only of complications like perforation or intestinal obstruction. Contrast enhanced computed tomography may reveal asymmetrical thickening and inflammation of jejunal bowel loops, focal outpouchings filled with fecal material or localized free intra-peritoneal air adjacent to the thickened jejunum [11]. Conventional enteroclysis can demonstrate the diverticula but use is limited as it is contraindicated in patients with acute complications of the disease. Multislice CT has obviated need for enteroclysis in most cases [11]. Newer methods like capsule endoscopy and balloon enteroscopy are reported to be useful but they are expensive, invasive and contraindicated in acute cases with complications [12]. Diagnostic laparoscopy may be useful to evaluate patients with complicated symptomatology and may avoid need for formal laparotomy. Many times, though, the diagnosis is made only on laparotomy. In our case, the diagnosis of perforation peritonitis was made on x-ray of abdomen in erect position.
Management of jejunal diverticular perforation varies depending on the degree of peritoneal contamination and patient’s condition. Novak reported that nonsurgical management with intravenous antibiotics and supportive measures along with percutaneous CT-guided aspiration of intraperitoneal collections may be appropriate for stable patients with localized peritonitis [13]. However, in case of generalized peritonitis with perforated diverticulum, emergent laparotomy with segmental bowel resection and primary anastomosis is the treatment of choice [14]. Extent of bowel resection required varies according to extent of diverticulosis. If extensive, then segments with grossly normal or non-inflammed diverticula may be left behind. This is to avoid short bowel syndrome due to extensive bowel resection. Simple diverticulectomy is not recommended as doing so would risk devascularizing the adjoining jejunal segment and cause anastomotic leakage and fistula formation [14]. Surgery for perforated diverticula carries a high morbidity and mortality, due to elderly population and associated comorbidities [1,5,7].
Conclusion
Diverticula of the jejunum are rare and are usually asymptomatic. They may lead to chronic abdominal symptoms or may present with complications like perforation. Complications in elderly patients may lead to significant morbidity and mortality, especially if diagnosis and therapy is delayed. Hence, in all cases of acute abdomen in elderly patients, jejunal diverticulosis and its complications like perforation must be included in the differential diagnosis. Emergent surgery is the treatment of choice once the diagnosis is made. Timely surgery can reduce the morbidity and mortality and provides the best outcome in these cases.
References
- Tsiotos GG, Farnell MB, IIstrup DM. Nonmeckelian jejunal or ileal diverticulosis: An analysis of 112 cases. Surgery. 1994;116:726-732.
- Akhrass R, Yaffe MB, Fischer C, Ponsky J, Shuck JM. Small-bowel diverticulosis: perceptions and reality. J Am Coll Surg. 1997;184:383-388.
- Wilcox RD, Shatney CH. Surgical implications of jejunal diverticula. South Med J. 1988, 81:1386-1391.
- Williams RA, Davidson DD, Serota AI, Wilson SE. Surgical problems of diverticula of the small intestine. Surg Gynecol Obstet. 1981;152:621-626.
- Longo WE, Vernava AM. Clinical Implications of Jejunoileal Diverticular Disease. Dis Colon Rectum. 1992;35:381-388.
- Ritvo M, Votta PJ. Diverticulosis of jejunum and ileum. Radiology. 1946;46:343-350.
- Baskin RH Jr, Mayo CW. Jejunal diverticulosis; a clinical study of 87 cases. Surg Clin North Am. 1952;1185-1196.
- Benson RE, Dixon CF, Waugh JM. Non-Meckelian diverticula of the jejunum and ileum. Ann Surg. 1943;118:377-393.
- Roses DF, Gouge TH, Scher KS, Ranson JH. Perforated diverticula of the jejunum and ileum. Am J Surg. 1976;132:649-652.
- Herrington JL Jr. Perforation of acquired diverticula of the jejunum and ileum- Analysis of reported cases. Surgery. 1962;51:426-433.
- Hyland R, Chalmers A. CT features of jejunal pathology. Clin Radiol. 2007;62(12):1154-1162.
- Carey EJ, Fleischer DE. Investigation of the small bowel in gastrointestinal bleeding- enteroscopy and capsule endoscopy. Gastroenterol Clin North Am. 2005;34(4):719-734.
- Novak JS, Tobias J, Barkin JS. Nonsurgical management of acute jejunal diverticulitis: a review. Am J Gastroenterol. 1997;92(10):1929-1931.
- Mattioni R, Lolli E, Barbieri A, D’Ambrosi M. Perforated jejunal diverticulitis: Personal experience and diagnostic with therapeutical considerations. Ann Ital Chir. 2000;71:95-98.