|
|
|
|
|
Pure Uterine Lipoma
|
|
|
Kuppili Venkata Murali Mohan1, Dabbiru Radhika2, Chakkirala Nalini Mohan1, Sanakkayala Rajkumari3, Jukuri Naganarasimha Raju4
From the Departments of Pathology1, Obstetrics & Gynaecology3, Radiology4, Katuri Medical College, Guntur, Andhra Pradesh and Department of Anatomy2, Guntur Medical College, Guntur, Andhra Pradesh, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. K.V. Murali Mohan
Email: kuppilimm@gmail.com
|
|
|
|
|
|
|
|
|
Received:
19-DEC-2014 |
Accepted:
24-DEC-2014 |
Published Online:
15-JAN-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Pure uterine lipoma is an uncommon benign mesenchymal neoplasm. It is generally seen in postmenopausal women presenting with abdominal pain. We describe a case of 70 year old woman who presented with abdominal pain and was diagnosed as uterine lipoma. |
|
|
|
|
|
Keywords :
|
Lipoma, Abdominal Pain, Neoplasms, Postmenopause, Uterus, Humans.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffd407060000005003000001000500 6go6ckt5b5idvals|415 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Lipomatous tumors of the uterus are rare benign neoplasms usually mixed with other mesenchymal neoplasms. Pure uterine lipoma – also named as “uterine fatty tumor” – usually occurs in postmenopausal women 50 to 70 years of age [1-4]. Incidence varies from 0.03-0.2%. These are often misdiagnosed as malignancy in view of presentation in later age. Most of the patients are asymptomatic. The signs and symptoms are similar to those caused by leiomyomas of the same size such as palpable mass, excessive menstrual bleeding and pelvic pain [5]. Uterine lipoma should be included in differential diagnosis of postmenopausal women presenting with abdominal pain or menorrhagia.
Case Report
A 70 year old woman was admitted with a complaint of pain abdomen. Pain was insidious in onset, gradually progressive, dull aching and non-radiating. She was postmenopausal with regular menstrual cycles in the past. On examination, her vitals were stable. On per abdomen examination, no mass was felt. Cervix, vagina were healthy on vaginal and per speculum examination. Routine investigations including carcinoma antigen-125 (CA-125), carcino embryonic antigen (CEA) & alfa-feto protein (AFP) were in normal range.
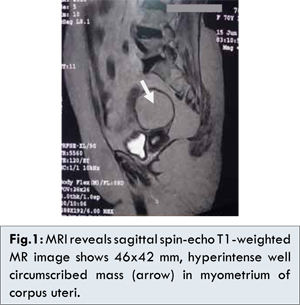
Ultrasound scan showed hyperechoic and homogenous space occupying lesion of size 5.8x4.6 x5.6 cm, in left adnexa abetting the uterus. MRI confirmed presence of well defined, round mass lesion 4.6x4.2x4.4 cm which was hyperintense on T1, isointense on T2 and suppressed on Short Tau Inversion Recovery (STIR) images suggesting fat containing lesion. Uterus was atrophic with mass in centre. Planes between mass & uterus were not clearly defined [Fig.1].
Total abdominal hysterectomy and salpingo-oopharectomy was done. On gross examination the uterus weighed 250 grams and measured 6x4x3 cm. The uterus body show left sided circumscribed mass of 4.5 cm, arising from wall of uterine fundus. Cut section show yellowish greasy tumor mass. Fallopian tubes and ovaries did not show any significant pathology [Fig.2]. Multiple sections were processed and stained with Hematoxylin & Eosin. The sections show lobules of mature adipocytes separated by thin vascular connective tissue. The myometrium was pushed to periphery forming a pseudo-capsule with atrophic endometrium. Histopathology confirmed the diagnosis of pure lipoma [Fig.3,4].
Discussion
Lipomas are defined as encapsulated adipose tissue with thin septa of fibrous tissue with smooth muscles confined to the periphery of the tumor [6]. Lipomatous tumors can be subdivided into pure lipoma, mixed lipoma and liposarcoma [3].
Various hypothesis that have been put forward to explain development of pure uterine lipoma include (i) misplaced embryonic mesodermal retaining potential for lipoblast differentiation. (ii) totipotent mesenchymal cell transformation. (iii) metaplasia of smooth muscle into adipose cells. (iv) perivascular fat cells proliferation [1,3]. Tumor typically appears as a well-defined homogenously hyperechoic lesion on ultrasound with surrounding hypoechoic rim representing adjacent compressed myometrium [3,7]. MRI is best modality for determining internal architecture of a tumor and the presence of fat [8]. MRI is modality of choice because of its multi planner capability and its ability to demonstrate fat component of the lesion. It is essential to differentiate lipomatous uterine tumors from other lesions especially ovarian teratoma which requires surgical intervention [3]. The woman described in this case report was 70 year old postmenopausal who presented with abdominal pain. Preoperative diagnosis was made by MRI and was pathologically confirmed postoperatively.
Conclusion
Pure uterine lipoma is very rare, however, awareness is the key to diagnosis and appropriate management. MRI and Hemotoxylin and Eosin staining may be helpful. Optimal management avoids unnecessary surgery and provides a good outcome.
References
- Imenpour H, Petrogalli F, Anselmi L. Pure uterine lipoma. Journal of the Italian society of anatomic pathology and diagnostic cytopathology 2013;105:24-27.
- Pounder DJ. Fatty tumors of the uterus. J Clin Pathol. 1982;35:1380-1383.
- Chu CY, Tang YK, Augustine Chan TS, Wan YH, Fung KH. Diagnostic challenge of lipomatous uterine tumors in three patients. World J Radiol. 2012;4(2):58-62.
- Bandopadhyay A, Ray S, Bera P, Gangopadhyay M, Chakrabarti I, Dey B. Calcified pure uterine lipoma mimicking myoma. J Turkish-German Gynecol Assoc. 2010; 11:113-114.
- Singh R, Kumar B, Bhat RV, Dorairajan G. Uterine Lipoleiomyomas: a report of two cases with a brief review of literature. Journal of Clinical and Diagnostic Research 2012; 6(4):718-719.
- Fernandes H, Naik CN, Swethadri GK, Bangera I, Miranda D. Pure lipoma of the uterus: a rare case report. Indian J Pathol Microbiol 2007;50(4):800-801.
- Venkatanarasimha N, Dubbins PA, Freeman SJ. Incidental uterine mass. Br J Radiol. 2009; 82(984):1043-1045.
- Fujimoto Y, Kasai K, Furuya M, Honda N, Tojo R, Saito S, et al. Pure uterine lipoma. Journal of Obstetrics and Gynecology Research. 2006; 32(5):520-523.
- Vamseedhar A, Sivalingappa DB, Suresh DR, Geetha RL. Primary pure uterine lipoma: a rare case report with review of literature. Indian Journal of Cancer. 2011;48(3)385-387.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Murali Mohan KV, Radhika D, Mohan CN, Rajkumari S, Raju JNPure Uterine Lipoma.JCR 2015;5:16-18 |
|
Murali Mohan KV, Radhika D, Mohan CN, Rajkumari S, Raju JNPure Uterine Lipoma.JCR [serial online] 2015[cited 2026 May 21];5:16-18. Available from: http://www.casereports.in/articles/5/1/Pure-Uterine-Lipoma.html |

|
|
|
|
|