|
|
|
|
|
Sustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma
|
|
|
symbicort asthma inhaler symbicort generic
B. P. Poddar Hospital & Medical Research Ltd., 71/1, Humayun Sarani, New Alipore, Block-G, Kolkata- 700053. |
|
|
|
|
|
Corresponding Author:
|
Dr. Chanchal Goswami
Email: drcgoswami@gmail.com
|
|
|
|
|
|
|
|
|
Received:
04-MAY-2015 |
Accepted:
02-JUN-2015 |
Published Online:
30-JUN-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Introduction: Chromophobe renal cell carcinoma is universally accepted as a distinct subtype of renal cell carcinoma. There are conflicting reports on prognosis, and few data on response to treatment exist. Currently, we do not have any effective treatment for the metastatic disease apart from surgical procedures. We report unexpectedly high efficacy of temsirolimus in a patient, with metastatic chromophobe renal cell carcinoma of right kidney. Case Report: We present the case of a 50-year-old female patient with advanced chromophobe renal cell carcinoma of right kidney, relapsing after radical nephrectomy; she was diagnosed of mRCC (metastatic renal cell carcinoma) with multiple lung metastasis. Treatment with temsirolimus resulted in a stable disease for 48 cycles. Conclusion: Mammalian target of rapamycin inhibitors like temsirolimus have been an option in the management of such cases. The case presented here impresses that temsirolimus could be a viable option for patients with metastatic chromophobe renal cell carcinoma. |
|
|
|
|
|
Keywords :
|
Renal Cell Carcinoma, Kidney Neoplasms, Nephrectomy, Temsirolimus, mTOR inhibitor.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffe84f07000000f103000001000800 6go6ckt5b5idvals|482 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Renal cell carcinoma (RCC) accounts for approximately 1% of all cancers [ 1], and the incidence of kidney cancer, unlike other genitourinary malignancies, is rapidly increasing at 2.5% per year [ 1]. Chromophobe RCC (ChRCC) represents 5% of neoplasms of renal tubular epithelium [ 1]. ChRCC is a distinct type of renal cancer, is presumably derived from the intercalated cells of the collecting duct system, and exhibits a better prognosis than other types of RCC.
An enhanced understanding of the underlying biology of RCC has led to systemic therapy targeted at the vascular endothelial growth factor (VEGF) pathway as well as the mammalian target of the rapamycin (mTOR) pathway. Agents blocking these pathway elements have demonstrated robust efficacy, offer new strategic options for patients with metastatic RCC, and have largely replaced cytokines as the standard of care in this disease. Both drugs have been approved by the US Food and Drug Administration for the treatment of metastatic RCC. Data regarding the activity of sunitinib and sorafenib in advanced ChRCC are lacking because recent trials were restricted mostly to patients with clear cell renal cell carcinoma. In this report, we describe the case of a patient who had ChRCC and who experienced improvement in his general condition and stable disease on treatment with temsirolimus, suggesting temsirolimus as an effective and appropriate treatment for this metastatic RCC tumor subtype.
Case Report
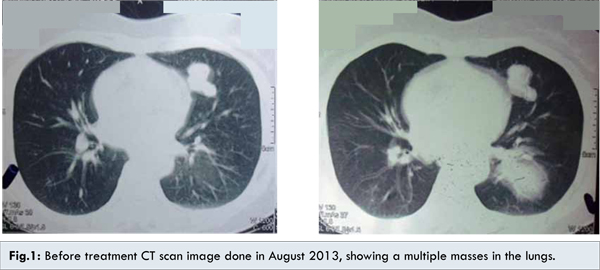
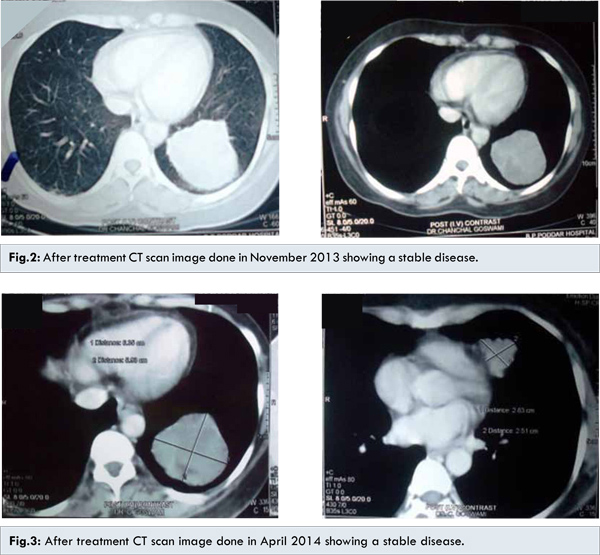
A 50-year-old female was diagnosed with renal cell carcinoma and further she underwent right radical nephrectomy in 2001. The tumor was limited to her kidney. The sections stained by hematoxylin and eosin showed sheets of polygonal cells with abundant granular eosinophilic cytoplasm with oval nuclei, convoluted nuclear membranes, and perinuclear cytoplasmic vacuolization. Histology revealed ChRCC. Twelve years after nephrectomy, patient was asymptomatic and lung metastasis was seen during routine follow up scans. The disease was considered advanced with multiple metastases to the lungs [Fig.1]. Since chromophobe cell variant, unlikely to benefit from VEGF-TKI, she was started on temsirolimus 25 mg weekly as intravenous infusion. After cycle 12th [Fig.2] and 24th [Fig.3], CT scan evaluation shows stable disease.
Patient has gone to receive 48 cycles of temsirolimus with a sustained stable disease. To the best of our knowledge, this case is the first report of ChRCC showing sustained response mTOR inhibitor therapy.
Discussion
RCC treatment has been classically derived from clinical trials that incorporated all histologies comprising clear cell, papillary, chromophobe, and other rarer subtypes. Most recently, novel therapies (sunitinib and sorafenib) have shown significant clinical activity in advanced RCC and have changed the standard of care in this disease [ 2- 4]. However, pivotal studies with these drugs were performed mostly in patients with clear cell histology. Therefore, the optimal therapy for papillary and chromophobe histologies remains unknown. Overall, ChRCC is considered to portend a good prognosis and is associated with earlier-stage tumors and longer overall survival in comparison with clear cell RCC. There are conflicting reports on prognosis in metastatic disease, and few data on response to treatment exist. Increased VEGF-6 and c-Kit (i.e., mast/stem cell growth factor receptor; proto-oncogene c-Kit; tyrosine-protein kinase Kit; or CD117) expressions have been reported in ChRCC, but the relevance of this to treatment is unknown [ 5- 7]. In an expanded-access trial of sunitinib, 13% of patients had non-clear cell histology, and there was evidence of clinical activity in this group [ 8]. A large international study reported the outcome of 1001 patients with metastatic RCC (82 of whom had papillary histology). Five year survival rates of papillary and clear cell subtypes were similar (about 10%). No treatment has proven to be active in papillary RCC, unlike clear cell renal cell carcinoma (ccRCC). One recently published series illustrated a response rate of only 5% in patients treated with these VEGF-targeted therapies [ 9]. Both responders received sunitinib, corresponding to an overall response rate of 17% in sunitinib-treated patients. Similarly, progression-free survival seemed to be longer in the patients treated with sunitinib in comparison with the patients treated with sorafenib (11.9 versus 5.1 months, respectively). Although the overall duration of follow-up was relatively short, the results support the clinical rationale for continued targeting of the VEGF and c-Kit signaling pathways in non-clear cell RCC [ 10, 11]. Choueiri and colleagues [ 12] retrospectively reviewed the efficacies of sunitinib and sorafenib in patients with metastatic papillary RCCs and ChRCCs. Seven patients with ChRCC were treated with sunitinib, and five were treated with sorafenib. A partial response occurred in three patients (25%), and the median progression-free survival time for patients with ChRCC was 10.6 months [ 12].
A phase III trial of temsirolimus also included patients with non-clear cell histology, and a subgroup analysis demonstrated an improved overall survival on temsirolimus in comparison with interferon and the combination of both drugs in ChRCC [ 13]. In this trial 626 patients with previously untreated, poor-prognosis metastatic renal-cell carcinoma were randomized to evaluate the overall survival in comparisons of the temsirolimus group and the combination-therapy group with the interferon group. Patients who received temsirolimus alone had longer overall survival (P=0.008) and progression-free survival (P<0.001) than did patients who received interferon alone. Overall survival in the combination-therapy group did not differ significantly from that in the interferon group (hazard ratio, 0.96; 95% CI, 0.76 to 1.20; P=0.70). Median overall survival times in the interferon group, the temsirolimus group, and the combination-therapy group were 7.3, 10.9, and 8.4 months, respectively. There were fewer patients with serious adverse events in the temsirolimus group than in the interferon group (P=0.02).
Personal experience reflects that VEGFR-TKI therapies have a variable response in these cancers and certain cancers fail to respond to this therapy. MTOR inhibitors are the other viable option with a slightly better response in ChRCC and this case report has helped to impress on temsirolimus as a viable and a feasible therapeutic option in the management of metastatic ChRCC.
Conclusion
In this report, we describe the case of a patient who had ChRCC and who experienced a prolonged improvement in his general condition and stable disease on treatment with temsirolimus and suggests that mTOR-targeted agents such as temsirolimus is effective and an appropriate treatment for this RCC tumor subtype. Now that agents directed against these pathways have largely replaced immunotherapy as the standard of care, new questions have emerged and are the subject of ongoing clinical trials. Additional prospective studies and clinical experience with this rare histologic nonclear cell subtype are needed.
References
- American cancer society. Kidney Cancer (Adult) - Renal Cell Carcinoma. Accessed from: http://www.cancer.org/acs/groups/cid/documents/webcontent/003107-pdf.pdf. [Accessed on 25 Mar 2015].
- Motzer RJ, Bacik J, Mariani T, Russo P, Mazumdar M, Reuter V. Treatment outcome and survival associated with metastatic renal cell carcinoma of non-clear-cell histology. J Clin Oncol. 2002;20:2376-2381.
- Cindolo L, de la Taille A, Schips L, Zigeuner RE, Ficarra V, Tostain J, et al. Chromophobe renal cell carcinoma: comprehensive analysis of 104 cases from multicenter European database. Urology. 2005;65:681-686.
- Beck SD, Patel MI, Snyder ME, Kattan MW, Motzer RJ, Reuter VE, et al. Effect of papillary and chromophobe cell type on disease-free survival after nephrectomy for renal cell carcinoma. Ann Surg Oncol. 2004;11:71-77.
- Jacobsen J, Grankvist K, Rasmuson T, Bergh A, Landberg G, Ljungberg B. Expression of vascular endothelial growth factor protein in human renal cell carcinoma. BJU Int. 2004;93:297-302.
- Escudier B, Eisen T, Stadler WM, Szczylik C, Oudard S, Siebels M, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;2:125-134.
- Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukowski RM, Rixe O, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007; 2:115-124.
- Gore ME, Szczylik C, Porta C, Bracarda S, Bjarnason GA, Oudard S, et al. Safety and efficacy of sunitinib for metastatic renal-cell carcinoma: an expanded-access trial. Lancet Oncol. 2009;10:757-763.
- Ronnen EA, Kondagunta GV, Ishill N, Spodek L, Russo P, Reuter V, et al. Treatment outcome for metastatic papillary renal cell carcinoma patients. Cancer 2006;11:2617-2621.
- Memeo L, Jhang J, Assaad AM, McKiernan JM, Murty VV, Hibshoosh H, et al. Immunohistochemical analysis for cytokeratin 7, KIT, and PAX2: value in the differential diagnosis of chromophobe cell carcinoma. Am J Clin Pathol. 2007;2:225-229.
- Patard JJ, Leray E, Rioux-Leclercq N, Cindolo L, Ficarra V, Zisman A, et al. Prognostic value of histologic subtypes in renal cell carcinoma: a multicenter experience. J Clin Oncol. 2005;12:2763-2771.
- Choueiri TK, Plantade A, Elson P, Negrier S, Ravaud A, Oudard S, et al. Efficacy of sunitinib and sorafenib in metastatic papillary and chromophobe renal cell carcinoma. J Clin Oncol. 2008;26:127-131.
- Hudes G, Carducci M, Tomczak P, Dutcher J, Figlin R, Kapoor A, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med. 2007;356:2271-2281.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Goswami C, Mandal ASustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma.JCR 2015;5:280-284 |
|
Goswami C, Mandal ASustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma.JCR [serial online] 2015[cited 2025 Jul 16];5:280-284. Available from: http://www.casereports.in/articles/5/1/Sustained-Response-to-Temsirolimus-in-Chromophobe-variant-of-Metastatic-Renal-Cell-Carcinoma.html |

|
|
|
|
|