Introduction
Ovarian fibroma is the commonest benign tumor of the ovarian stroma (3% of all ovarian neoplasms), and can be seen in any age [
1]. The cellular subtype, approximately 10% of ovarian fibromatous tumors, exhibit hypercellularity, increased mitotic activity, and mild-to-moderate nuclear atypia [
2]. The cellular fibroma is a tumor of uncertain malignant potential that may recur or be associated with peritoneal implants. The degree of mitotic activity is the main parameter for differentiating cellular fibroma from fibrosarcoma [
2,
3]. Fibrosarcomas usually exhibit moderate-to-severe nuclear atypia and mitotic counts of 4 or more per 10 high-power fields (HPFs). Macroscopically, the cellular fibroma resembles uterine leiomyoma in whitish appearance solid consistency and areas of cystic degeneration and stromal edema. Clinically, it is asymptomatic and may typically be detected during routine gynecological examinations. It is usually benign, but the completeness of excision and presence or absence capsule rupture are important prognostic parameters. We hereby report a 42 year old female having severe abdominal pain which was diagnosed as ovarian fibroma with torsion.
Case Report
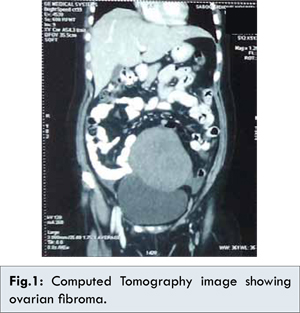
A 42 year old multiparous female came to our institute with complaint of pain in abdomen since 2 weeks. Her general condition was fair, pulse rate 72 beats/min and blood pressure 120/80 mmHg. Her respiratory and cardiovascular system examination findings were within normal limits. Abdomen examination revealed, a huge mass corresponding to 24-26 weeks uterine size, arising from the lower pelvis and extending upwards. The mass was hard in consistency, nontender with restricted mobility and its lower border could not be reached. On per speculum examination, her cervix was hypertrophied, with erosions present circumferentially. On per vaginal examination, abdomen findings were confirmed to 24-26 weeks size palpable mass with restricted mobility and uterus was not separately palpable, bilateral forniceal fullness was present with no tenderness. Her routine blood and urine investigations were within normal limits. Pap smear was suggestive of inflammatory smear with no evidence of malignancy. Her tumor markers were as follows: CA 125 was 27.45 IU/mL (normal values 0-35 IU/mL), carcino embryonic antigen was 0.867 ng/mL (normal values 0-2.5 ng/mL), alpha fetoprotein was 0.92 IU/mL (normal values 0-5.2 IU/mL), CA 19.9 was 11.3 U/mL (0-35 U/mL). She had normal chest X-ray while her ultrasound abdomen with pelvis was suggestive of approximately 12.3 cm x 11.4 cm sized mixed echogenicity mass in left adnexal region Her Computed Tomography image (CT scan) was suggestive of 12.3 cm x 10 cm x 12.5 cm solid lesion in pelvis mainly in left adnexa extending upto supraumbilical region with heterogenous enhancement with minimal post contrast enhancement [Fig.1,2]. Her provisional clinical diagnosis was of ovarian tumor. Exploratory laparotomy was done and specimen sent for frozen section. In situ there was mild free fluid present, there was large left ovarian solid mass approximately 14 cm x 14 cm × 12 cm, hard in consistency with smooth surface having congested and thrombosed serosal vessels [Fig.3,4]. There was one and half turn torsion of ovarian ligament with fallopian tube, uterus was normal in size and shape, cervix was thick and elongated. Right side ovary and tube were grossly normal. Ovarian tumor pedicle was clamped, cut and ligated at the base and sent for frozen section histopathology. In view of frozen section report suggestive of benign ovarian fibroma, total abdominal hysterectomy with right salpingoophorectomy was done. The patient withstood the precedure well and was later discharged in healthy condition with final histopathology report suggestive of ovarian fibroma. Gross specimen revealed well encapsulated, greyish white, firm ovarian mass 13 cm x 12 cm x 8 cm. Microscopic features revealed tumor cells arranged in diffuse sheets and at places showing sporiform pattern. Individual tumor cells were spindle shaped with moderate amount of eosinophillic cytoplasm with oval to spindle nuclei [Fig.5,6]. Endometrium was suggestive of proliferative phase, myometrium suggested leiomyoma, cervix showed chronic papillary endocervicitis with nabothian cyst, right ovary was suggestive of corpus albicans, congested blood vessels and both fallopian tubes had congested serosa. Final histopathology report was suggestive of ovarian fibroma.
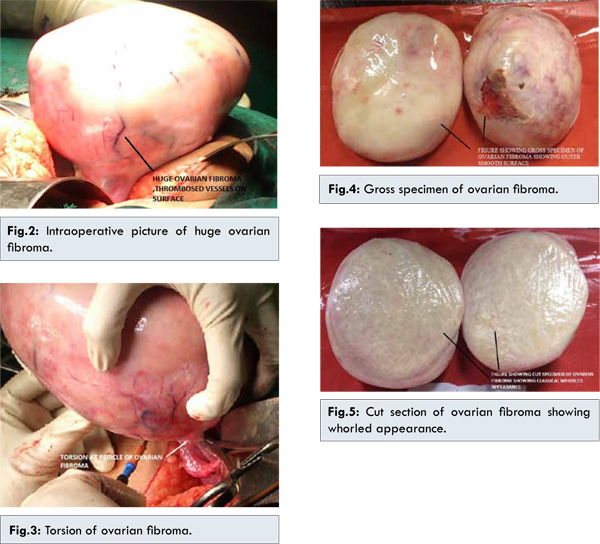
Our patient was 42 year old female who presented with abdominal pain without any history of any nausea, vomiting or any altered bowel or bladder habits. There was hard, immobile, nontender 24 weeks to 26 weeks uterine size mass arising from the pelvis with nonpalpable lower border. Tumor markers CA-125, CEA, alpha fetoprotein values were within normal limits. In situ, tumor was having torsion with classical gross appearance being solid consistency, smooth surface with congested and thrombosed veins and was mimicking benign ovarian fibroma [Fig.5]. The right ovarian fibroma associated with hydrothorax and ascitis is classified as Meig’s syndrome, but in our case there was minimal ascitis but no pleural effusion.
Cellular fibromas are predominantly solid. Cystic areas are usually small and without multiloculation. Few fibromas may undergo prominent cystic degeneration and may be misdiagnosed as surface epithelial stromal tumors. However, the cyst (pseudocyst) do not have an epithelial lining [
4,
5]. However, cellular fibroma is a tumor of uncertain malignant potential. It is capable of locally aggressive growth if incompletely excised [
2]. Complete removal of tumor and mitotic count are prognostic markers of ovarian fibroma [
2]. Irving et al. [4] studied 75 cases of cellular fibromas of the ovary and suggested the term “mitotic active cellular fibroma (MACF)” to cellular fibromatous neoplasm with bland cytology with = 4 mitosis/10?HPF. They pointed out that the term fibrosarcoma should be reserved for fibroblastic tumour with moderate or severe atypia and high mitotic activity. This patient withstood surgery well and her postoperative period was uneventful.
Conclusion
While most of the patients with ovarian fibroma remain asymptomatic, patient can present with acute abdomen due to torsion. In a case presenting with acute abdomen with lump abdomen, ovarian mass with torsion should be kept as differential diagnosis.
References
- Padubidri VG, Shirish N Daftary SN. Shaws textbook of Gynecology, 16th Edition. New Delhi: Reed Elsevier; 2015. pp.521-530.
- Prat J, Scully RE. Cellular fibromas and fibrosarcoma cases. Cancer. 1981;47(11):2663-2670.
- Young RH. Sex cord-stromal, steroid cell, and other ovarian tumors with endocrine, paraendocrine, and paraneoplastic manifestations. In: Kurman RJ, Ellenson LH, Ronnett BM (eds.). Blaustein’s Pathology of the Female Tract, 6th edition. New York; Springer;2011. pp.785-846.
- Irving JA, Alkushi A, Young RH, Clement PB. Cellular fibromas of the ovary: a study of 75 cases including 40 mitotically active tumors emphasizing their distinction from fibrosarcoma.American Journal of Surgical Pathology. 2006;30(8):929-938.
- Katke RD. Successful Outcome of Pregnancy in Borderline Malignant Ovarian Tumor. Journal of Case Reports. 2014;4(2):391-394.