Introduction
Neuroendocrine tumors of the female genital tract, either primary or secondary are rare [
1]. Carcinoid tumors account for approximately 2% of metastatic ovarian neoplasms [
2]. Ovarian metastases are bilateral in approximately 70% of cases [
3].Malignant tumors that metastasize to the ovary from extra-ovarian primary neoplasms are categorised as secondary tumors of the ovary. Tumors that extend to the ovary directly from adjacent organs or tissues are also included in this category [
3]. We present a rare association of unilateral borderline mucinous cystadenoma of ovary with a metastasis by direct extension from an ileal neuroendocrine tumor.
Case Report
A 50 year old female presented with the chief complaints of pain abdomen since 15 days. Previous medical history was unremarkable. Routine laboratory investigations were normal. Ultrasound abdomen and CT scan abdomen revealed 4.5x3.8 cm well defined left ovarian cyst. During laparotomy, an ileal growth was identified. Ileal resection, anastomosis and bilateral oophorectomy were done. We received two specimens.
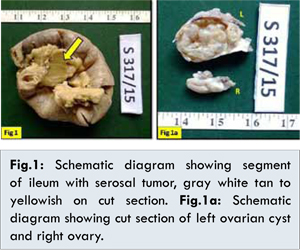
Specimen I-A segment of small intestine of length 16 cm, showed two polypoidal masses of 4x2.5x2 cm and 2x2x1 cm diameter respectively, on the serosal aspect. The overlying mucosa was intact. Cut section of polypoidal mass was homogenously gray white, tan to yellowish [Fig.1]. Specimen II was bilateral salpingo-ophorectomy specimens with left ovarian mass of size 5x4x2 cm with attached tube of 2 cm. External surface was nodular. Cut section showed solid and cystic areas with an yellowish area near surface. Right side ovary was of size 4x1.5x0.5 cm [Fig.1a].
Sections from small intestine showed normal ileal mucosa [Fig.2]. Sections from both the polypoidal masses on ileal serosa, showed a tumor composed of uniform round to oval cells, with regular monomorphic nuclei, stippled chromatin and inconspicuous nucleoli arranged in insular pattern with peripheral palisading located in the ileal submucosa [Fig.2,2a], suggesting a neuroendocrine tumor. Sections from left ovary showed tumor lined by columnar mucinous cells (intestinal type) and rounded cells with eosinophilic cytoplasm which are stratified with detached cell clusters [Fig.2b]. The histological picture is suggestive of a borderline mucinous cystadenoma along with a surface implant from neuroendocrine tumor [Fig.2c].
A diagnosis of “neuroendocrine tumor of small intestine with evidence of metastasis in left ovary associated with a borderline mucinous cystadenoma” was made. After surgery, the patient has been asymptomatic during her follow up for ongoing chemotherapy.
Discussion
According to Lopes Dias et al. the median age of diagnosis is 55 years (range from 17 to 83 years), with most of the patients being peri- or postmenopausal [
1]. According to Marianne Pavel and Ashley Grossman et al. in two reports of 17 and 35 cases, the median age at the time of detection of ovarian metastases was 57 years (range 44-77 and 21-82, respectively) [
4]. The size of the ovarian lesions varies and may range from microscopic foci to lesions 1.9 cm in size. Approximately 30% are identified at autopsy [
4]. Approximately 2% of small intestinal neuroendocrine tumors greater than 1 cm in diameter spread to the ovary. They are usually bilateral in contrast to primary ovarian lesions, which are usually unilateral. Although most metastatic carcinoids are of small intestinal origin, rarely the primary tumor originates in the appendix, colon, stomach, pancreas, or lung [
2].
Carcinoid tumor of the ovary may be primary or metastatic. Primary carcinoids are subdivided into four categories: (i) insular, (ii) trabecular, (iii) strumal, and (iv) mucinous. Mixed types also occur (composed of any combination of the pure types). The latter are uncommon and often associated with a mature cystic teratoma. Of the metastatic carcinoids, the insular carcinoid tumor is the most common, followed by the trabecular and mucinous types [
2]. According to the literature, the insular and trabecular subtypes most commonly have metastases in the ovary simulating a primary tumour. The present case showed insular pattern in correlation with the literature. Metastatic carcinoid is nearly always bilateral [
5]. Robboy et al. compared the features of primary insular carcinoids and metastatic midgut carcinoids and concluded that the presence of extra-ovarian tumour, bilaterality, multinodularity, vascular invasion and the absence of teratomatous elements are suggestive of an extra-ovarian origin [
1]. The present case showed unilateral metastasis and there were no teratomatous elements.
The routes of tumor spread to the ovary are variable. Lymphatic and hematogenous metastasis to the ovaries is the most common form of dissemination. Direct extension is also a common manner of spread from adjacent tumors of the fallopian tube, uterus and colorectum [
3]. The identification of surface implants, multinodularity and intravascular tumor emboli are extremely helpful histological clues in the recognition of secondary ovarian tumors that spread through the abdominal cavity and tubal lumen [
3]. In the present case, presence of surface implant in one side ovary is an important histological evidence for the tumor spread.
Cardiac and ovarian metastases are more commonly associated with carcinoid syndrome. The present case showed no carcinoid syndrome symptoms. In 35 patients with ovarian metastases, a 5-year survival rate of 25% was reported in 1974, while a recent report indicates a projected 5-year survival of 94% [
4].
Conclusion
We present a rarest association of unilateral borderline mucinous cystadenoma of ovary with a metastasis by direct extension from an ileal neuroendocrine tumor.
References
- João Lopes Dias, Teresa Margarida Cunha, Filipe Veloso Gomes, Catarina Callé, Ana Félix. Neuroendocrine tumours of the female genital tract: a case-based imaging review with pathological correlation. Insights Imaging. 2015; 6:43-52.
- Melinda F. Lerwill, Robert H. Young. Metastatic Tumors of the Ovary. In: Kurman RJ, Ellenson H, Lora, Ronnett BM editors. Blaustein’s Pathology of the Female Genital Tract, 6th edition. New York: Springer; 2011. pp.930-990.
- Prat J, Morice G. Secondary tumors of ovary. In: Tavassoli FA, Peter Devilee P. editors. World Health Organization Classification of Tumors. Pathology and Genetics of Tumors of the Breast and Female Genital Organs. IARC Press: Lyon 2003. pp.194-196.
- Pavel M, Grossman A, Arnold R, Perren A, Kaltsas G, Steinmüller T, et al. ENETS Consensus Guidelines for the Management of Brain, Cardiac and Ovarian Metastases from Neuroendocrine Tumors: Neuroendocrinology. 2010;91:326-332.
- Strosberg J, Nasir A, Cragun J, Gardner N, Kvols L. Metastatic carcinoid tumor to the ovary: a clinicopathologic analysis of seventeen cases. GynecolOncol. 2007;106(1):65-68.