Introduction
Spigelian hernia refers to protrusion of pre-peritoneal fat and peritoneal sac through the Spigelian aponeurosis which may present with uncharacteristic abdominal pain and a palpable mass along the Spigelian aponeurosis [
1]. Spigelian hernias constitute nearly 0.12 % of all abdominal wall hernias and are associated with high risk of strangulation and gangrene [
2]. The diagnosis of Spigelian hernia presents greater difficulties than its treatment [
3]. The clinical presentation varies, depending on the contents of the hernial sac and the degree and type of herniation. Incarcerated Spigelian hernia is a rare cause of abdominal pain requiring emergency surgery [
4]. Ultrasound examination is a valuable diagnostic tool both in palpable and non-palpable Spigelian hernias [
3]. Surgical repair is the treatment of choice and is associated with very low recurrence [
5]. Our patient had obstructed Spigelian hernia.
Case Report
A 40 year old male presented in surgical emergency with an irreducible swelling in right lower quadrant of abdomen, colicky pain, constipation and progressive abdominal distension for 2 days. There was no history of trauma, previous surgery or tuberculosis.
He had tachycardia with normal blood pressure. Abdomen was distended with a vague, tender, globular lump of diameter 10 cm in right lumbar and umbilical region with normal local temperature, smooth surface, ill-defined margins. The lump was firm, had restricted mobility, prominent with leg raising test, irreducible with absent bowel sounds [Fig.1]. There was no feature of generalised peritonitis, no apparent organomegaly, external genitalia was normal and hernia sites were free. Digital per rectal examination showed ballooning along with scant faecal matter.

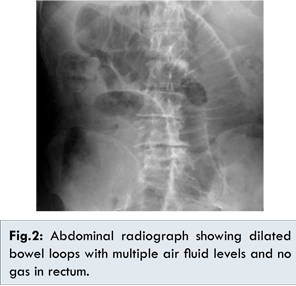
Blood investigations showed total leucocyte count to be 16,500 with relative neutrophilia. Rest of blood parameters along with organ function tests were normal. Abdominal radiograph showed dilated bowel loops with multiple air fluid levels with no gas in rectum [Fig.2]. Ultrasonography of abdomen showed dilated, aperistaltic bowel loops along with herniation of bowel loop through a wall defect present lateral to right rectus muscle nearly 4 cm below umbilicus. Rest of the viscera was normal.
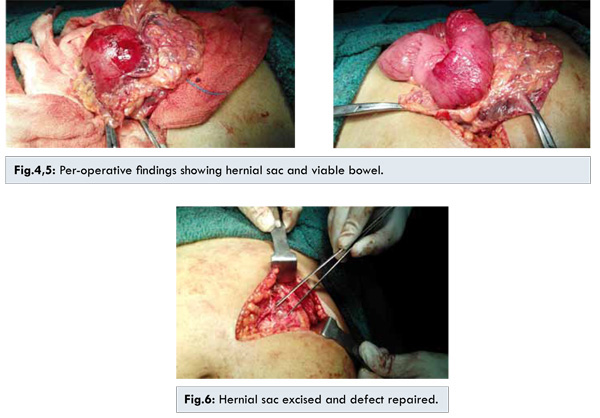
With a diagnosis of obstructed hernia, the patient was kept nil by mouth along with nasogastric tube placement and started on antibiotics, analgesics and intravenous fluids and was monitored intensively. After optimisation, surgical exploration was done through a curved transverse incision. Per-operatively we found a hernial sac with defect in Spigelian fascia containing bowel loop and mesentery along with inflammatory fluid [Fig.3]. The hernial sac was opened and toxic fluid was evacuated. The neck of the hernia defect was widened and viability of bowel ensured [Fig.4,5]. Healthy bowel was reduced after excision of gangrenous omentum. Hernial sac was excised and defect of size 2x2 cm was repaired primarily with polypropylene 1-0 suture and abdomen closed in layers with vicryl [Fig.6]. Mesh was not placed in view of small defect and possibility of infection.

Post-operatively, patient was kept nil by mouth for two days, on antibiotics and analgesics and recovery was smooth and was discharged on fifth post-operative day. He is asymptomatic at 10 months follow up.
Discussion
Although Spigelian hernia was thought to be unusual but they are not as uncommon as previously thought. It can occur at any position within the extent of Spigelian fascia. Unspecific and variable presentation makes it liable for misdiagnosis pre-operatively. Common presentations are intermittent mass, pain in lower abdominal region or features of bowel obstruction. Usually they are unilateral and left sided in old females. Risk factors include chronic cough, trauma, obesity, constipation, prior surgery, ascites, and sudden weight loss. Differential diagnoses are appendicitis, diverticular disease, Kochs abdomen, cholecystitis, colonic malignancy, ovarian disease, rectus sheath hematoma, focal abscess and other hernias [
6]. Our patient presented with typical features of obstructed hernia i.e. pain, constipation and abdominal distension along with irreducible tender abdominal lump and empty rectum.
Conventional radiography has limited role in giving etiological diagnosis. Ultrasonography [
7] is a good non-invasive, readily available modality which can diagnose this rare pathology. Contrast enhanced computerised tomography [
8] is standard investigation which diagnoses majority of cases and offers specific information for the abdominal defect, size, content of the sac and the relations with the surrounding tissues. Our diagnosis was based on clinical features, abdominal radiography and sonography.
Treatment of choice is surgical repair. Transverse incision is preferred to avoid damage to motor nerves. Grid iron approach to muscles and excision of hernia sac is done. The defect is repaired primarily with or without prosthetic mesh application depending on size of defect and contamination. Extra-peritoneal laparoscopic repair can also be done in elective cases with excellent results [
9]. Our patient underwent anterior open herniotomy with primary repair of defect without placement of mesh in view of emergency nature of indication and possible risk of infection. Complications like haematoma, focal abscess and ileus can occur but our patient had uneventful post-operative recovery.
Conclusion
Diagnosis of Spigelian hernia is challenging due to vague symptoms, low incidence and lack of clinical experience. High index of suspicion is needed to avoid high risk of complications.
References
- Kalaba Z1, Ugeskr Laeger. Spigelian hernia. A case of typical Spigelian hernia in an elderly man. 1999;161(14):2095-2096.
- 2.Spinelli C, Strambi S, Pucci V, Liserre J Spinelli G, Palombo C. Spigelian Hernia in a 14-Year-Old Girl: A Case Report and Review of the Literature. Eur J Pediatr Surg Rep. 2014;2:58-62.
- Spangen L. Spigelian hernia. World J Surg. 1989;13(5):573-580.
- Savikko J, Kokkola A. Incarcerated Spigelian hernia. Duodecim. 2012;128(5):518-522.
- Moreno Egea A, Carrasco L, Girela E, Martín JG, Aguayo JL, Canteras M. Open vs Laparoscopic Repair of Spigelian Hernia. Arch Surg. 2002;137(11):12661268.
- Habib E, Elhadad A. Spigelian hernia long considered as diverticulitis: CT scan diagnosis and laparoscopic treatment. Computed tomography. Surg. Endosc. 2003;17:159.
- Mufid MM, AbuYousef MM Kakish ME Urdaneta LF, Al Jurf AS. Spigelian hernia: diagnosis by highresolution realtime sonography. J Ultrasound Med. 1997;16:183.
- Shenouda NF, Hyams BB, Rosenbloom MB. Evaluation of Spigelian hernia by CT. J Comput Assist Tomogr. 1990;14:777.
- Novell F, Sanchez G, Sentis J, Visa J, Novell J, Novell-Costa F. Laparoscopic management of Spigelian hernia. Surg Endosc. 2000;14:1189.